Translate this page into:
Disseminated molluscum contagiosum infection in a hyper IgE syndrome
Correspondence Address:
Vidya Kharkar
Department of Dermatology, Seth G.S. Medical College and K.E.M Hospital, Parel, Mumbai 400 012, Maharashtra
India
| How to cite this article: Kharkar V, Kardekar S, Gutte R, Mahajan S, Thakkar V, Khopkar U. Disseminated molluscum contagiosum infection in a hyper IgE syndrome. Indian J Dermatol Venereol Leprol 2012;78:371-374 |
Sir,
Buckley et al., described the hyper IgE syndrome, also known as Job′s syndrome is a rare complex primary immune deficiency, characterized by multiple cutaneous infections, eczema, pulmonary infections, highly elevated serum IgE, various connective tissue, skeletal and vascular abnormalities. [1],[2]
Autosomal recessive hyper IgE syndrome (AR-HIES) manifests as severe eczema, recurrent bacterial and viral skin infection and they specifically lack connective tissue and skeletal manifestions. [1],[3]
A 10-year-old male child born of consanguineous marriage was brought with multiple gradually increasing asymptomatic pearly white raised lesions all over body since 6 months [Figure - 1] and [Figure - 2]. There was a past history of multiple, recurrent pus-filled lesions on his chest, groins along with recurrent pulmonary infections. There was no personal or family history of atopy. There was no history of any dental, skeletal, neurological problems or any distinctive facies. Out of three siblings, one younger sibling had history of similar skin lesions all over body.
 |
| Figure 1: Multiple pearly white umbilicated papules over face |
 |
| Figure 2: Multiple pearly white umbilicated papules and nodules over the chest |
Cutaneous examination revealed multiple pearly white papules and nodules with central umbilication and few pus-filled lesions on chest and groins. Bilateral inguinal lymphadenopathy with non-tender and non-matted nodes was seen [Figure - 3]. Rest of the cutaneous examination including nails, mucosae and hair was normal. Systemic examination was within normal limits.
 |
| Figure 3: Multiple pearly white umbilicated papules and nodules and inguinal lymphadenopathy |
On investigations, hemoglobin was 8 gm%, total leucocyte count was raised and differential count showed 27% eosinophils and absolute eosinophil count was 8689 cells/μl (Normal <700 cells/μl). Elisa for HIV was negative. Routine and microscopic examination of stool and urine was normal. Chest X-ray and ultrasound examination of abdomen was normal and Mantoux test was negative. Skin biopsy from a papule showed proliferation of epidermis with molluscum bodies suggestive of molluscum contagiosum [Figure - 4].
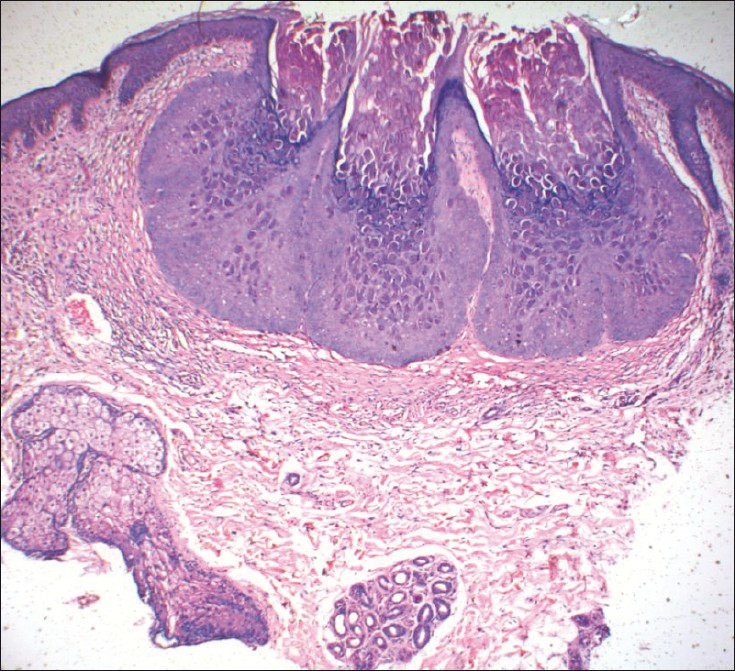 |
| Figure 4: Infundibular proliferation with multiple characteristic molluscum bodies. (H and E, ×40) |
On clinicopathological correlation, a diagnosis of hypereosinophilic syndrome with disseminated molluscum contagiosum was made. The bone marrow biopsy and computed tomography of abdomen showed no abnormality. On further workup, immunoglobulin level showed normal IgG, IgA and IgM but serum IgE level were highly elevated (12400 IU/ml). Nitroblue tetrazolium test was negative and C3, C4 complement levels were normal, however neutrophil chemotaxis studies could not be done. Absolute CD4 T cells count was 613/mm 3 and CD8 T cells was 253/mm 3 . According to National Institute of health scoring, patient had the score of 30 indicating that he is affected with HIES. [4]
Based on history, examination and histopathology a diagnosis of autosomal recessive hyper-IgE syndrome (AR- HIES) was made. The patient was treated with topical and oral antibiotics according to culture and sensitivity and large abscess were drained surgically. Extraction with curette was done for facial molluscum lesions and counseling of parents was done. However, later patient succumbed to pneumonia and hence we could not do any further follow-up.
Hyper IgE syndrome (HIES) with recurrent infections (Job′s syndrome) is a rare idiopathic primary immunodeficiency disease characterized by the triad of elevated serum IgE levels (>2000 IU/ml), recurrent cutaneous abscesses and recurrent sinopulmonary infections. [1]
HIES or Job′s syndrome was described in 1966 by Davis, Schallar and Wedgewood. In 1972 with reference to Biblical character Job who was smote with sore boils, the Buckley and colleagues refined the syndrome after detection of highly elevated serum IgE in conjunction with eczema and recurrent skin and pulmonary infections. [2]
Two types of hyper IgE syndrome are known, autosomal dominant and autosomal recessive. However, sporadic cases are also common. Autosomal dominant type is a rare multisystem disorder with connective tissue, skeletal and vascular abnormalities. AR-HIES is due to null mutation in tyrosine kinase 2 gene causing defect in innate and adaptive immunity and susceptibility eczemas, skin and pulmonary infection with increased serum IgE levels. Among viral infections, molluscum contagioum virus infection is the most common and skeletal and connective tissue abnormalities are absent. [2]
The etiology and pathogenesis of HIES is not completely understood and mechanisms responsible for increased production of IgE is not known. Recent research points toward a skewed T helper 1 (Th1) cell/Th2 cell ratio and the involvement of chemokines in its pathogenesis. Defects along the TH17 differentiation pathway is probably involved in genetically distinct forms of the hyper IgE syndrome. [5],[6]
Disseminated MC infection along with HIES, can occur in generalized eczema also. Yang et al., described a case with generalized chronic eczema with disseminated MC in 26 year old women. [7] However, compared to atopic dermatitis, HIES tends to affect scalp and axillae more commonly with highly elevated serum IGE, recurrent cold abscess and more severe lung damage. [8] Other viral infection like herpes simplex and human papilloma virus infection can also occur in HIES. [9]
In absence of definitive cure, therapy for HIES is directed mainly at prevention and management of infections with sustained systemic antibiotics and antifungals along with topical therapy for eczema and drainage of abscesses. Various treatment modalities used for disseminated MC infection in HIES include physical destruction or manual extrusion of lesions, cryotherapy, curettage, imiquimod and retinoids. Succesfull treatment with subcutaneous interferon-alpha has been reported. [10] Interferons, immunoglobulin supplementation, or low-dose cyclosporine-A has been reported to benefit selected patients, but they are not generally indicated. Patients who undergo regular monitoring and receive appropriate treatment may live beyond the age of 50 years. Death is often due to infectious complications. [5],[6]
Acknowledgment
We would like to thanks to Dr. Manisha from Department of cytogenetics under ICMR in our institute for performing immunological assay.
| 1. |
Chularojanamontri L, Wimoolchart S, Tuchinda P, Kulthanan K, Kiewjoy N. Role of Omalizumab in a patient with hyper-IgE syndrome and review of dermatologic manifestations. Asian Pac J Allergy Immunol 2009;4:233-6.
[Google Scholar]
|
| 2. |
Freeman AF, Holland SM. Clinical manifestations, etiology and pathogenesis of the hyper-IgE syndrome. Pediatr Res 2009;65:32-7.
[Google Scholar]
|
| 3. |
Heimall J, Freeman A, Holland SM. Pathogenesis of hyper IgE syndrome. Clin Rev Allergy Dermatol 2010;38:32-8.
[Google Scholar]
|
| 4. |
Grimbacher B, Schäffer AA, Holland SM, Davis J, Gallin JI, Malech HL, et al. Genetic linkage of hyper-IgE syndrome to chromosome 4. Am J Hum Genet 1999;65:735-44.
[Google Scholar]
|
| 5. |
Grimbacher B, Holland SM, Puck JM. Hyper-IgE syndromes. Immunol Rev 2005;203:244-50.
[Google Scholar]
|
| 6. |
Al Khatib S, Keles S, Garcia-Lloret M, Karakoc-Aydiner E, Reisli I, Artac H. Defects along the T(H)17 differentiation pathway underlie genetically distinct forms of the hyper IgE syndrome. J Allergy Clin Immunol 2009;124:342-8.
[Google Scholar]
|
| 7. |
Yang CH, Lee W, Jeffrey TS. Disseminated white papules-Quiz case. Arch Dermatol 2006;142:775-80.
[Google Scholar]
|
| 8. |
Dhar S. On Atopic Dermatitis. In: Valia RG, Valia AR, editors. IADVL Textbook of Dermatology. 3 rd ed. India: Bhalani Publishing House; 2008. p. 527-34.
[Google Scholar]
|
| 9. |
Lei XB, Geng SM, Zeng WH, Tann SS, Wang JM, Xiao SX. Unusual coexistence of molluscum contagiosum and verruca plana in a hyper-IgE syndrome. Int J Dermatol 2006; 45:1199-201.
[Google Scholar]
|
| 10. |
Kilic SS, Kilicbay F. Interferon-α treatment of molluscum contagiosum infection in a patient with hyperimmunoglobulin E syndrome. Pediatrics 2006;117:1253-5.
[Google Scholar]
|
Fulltext Views
5,396
PDF downloads
2,528





![[Figure - 1]](#fig_ijdvl_2012_78_3_371_95464_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2012_78_3_371_95464_f2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2012_78_3_371_95464_f3.jpg){kind=link}
![[Figure - 4]](#fig_ijdvl_2012_78_3_371_95464_f4.jpg){kind=link}