Translate this page into:
Dome-shaped nodules and scaly, verruciform plaques on the legs and feet
Correspondence Address:
Carmen Mar�a Alc�ntara-Reifs
Dermatology Department, Reina Sofía University Hospital, Avda. Menéndez Pidal S/N, 14004, Córdoba
Spain
| How to cite this article: Alc�ntara-Reifs CM, Salido-Vallejo R, Garnacho-Saucedo GM, Garc�a-Nieto AV. Dome-shaped nodules and scaly, verruciform plaques on the legs and feet. Indian J Dermatol Venereol Leprol 2019;85:226-228 |
Plaques on the Legs and Feet
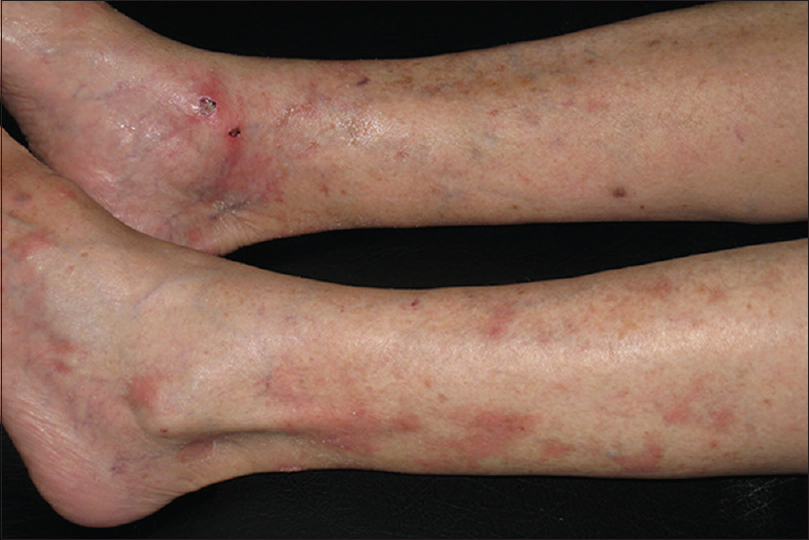
An 82-year-old woman was referred to our department for evaluation of itchy, scaly verruciform plaques on her legs of 3 years duration, previously diagnosed and treated as psoriasis without improvement. On examination, there were well-defined, erythematous scaly plaques and multiple verrucous, dome-shaped nodules on her legs and feet [Figure - 1] and [Figure - 2]. Routine blood tests were within the normal range, and antinuclear and anti-ds-DNA antibodies were negative. Histopathology showed hyperkeratosis, irregular acanthosis, follicular plugs, vacuolar interface change, and band like dermal lymphocytic infiltrate in a background of dermal mucin [Figure - 3].
 |
| Figure 1: Erythematous scaly plaques and multiple verrucous, dome-shaped nodules |
 |
| Figure 2: Keratoacanthoma-like papules and nodules on sun-damaged skin of the leg |
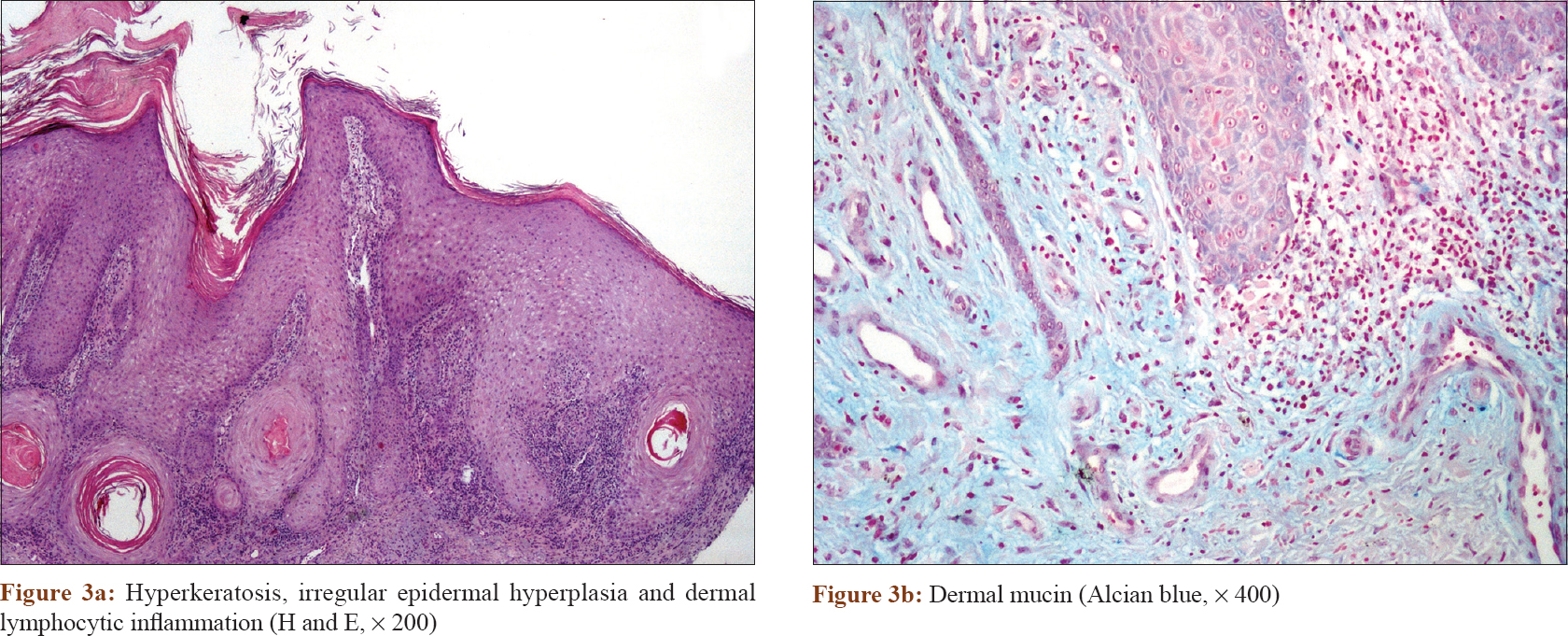 |
| Figure 3: |
Question
What is your diagnosis?
Diagnosis
Cutaneous hypertrophic lupus erythematosus (LE).
Discussion
Correlating the clinical and histological findings, a diagnosis of hypertrophic lupus erythematosus was made. The patient was treated with acitretin (25 mg/day) as monotherapy with significant improvement within 3 months [Figure - 4]. Hypertrophic lupus erythematosus is regarded as a distinct and rare subset of chronic discoid lupus erythematosus, representing 2% of all lesions of chronic cutaneous lupus erythematosus.[1] It is characterized by verrucous lesions due to an exaggerated proliferative epithelial response, in contrast to classical discoid lupus erythematosus. These lesions usually affect middle-aged females and are often chronic in course and resistant to treatment. A subset of patients with hypertrophic LE develops hyperkeratotic papules with central crater plugged with horny material, clinically and histologically reminiscent of keratoacanthomas.[2] On histopathology, most cases show irregular pseudoepitheliomatous hyperplasia, vacuolar interface changes and a dense, band-like infiltrate. Varying amounts of squamous atypia and necrotic keratinocytes may also be found which need to be differentiated from squamous neoplasia. Clinically, the development of verrucous plaques and keratoacanthoma-like nodules in patients of discoid lupus erythematosus suggests a diagnosis of hypertrophic lupus erythematosus. Microscopically, hyperkeratosis with follicular plugging, periadnexal and perivascular lymphocytic inflammation in a background of dermal mucin and basement membrane thickening, represent useful clues to the diagnosis of hypertrophic lupus erythematosus when present.[1],[3] In addition, Ko et al. have hypothesized that CD123-positive plasmacytoid dendrocytes can aid in the histopathologic distinction of hypertrophic lupus erythematosus from squamous cell carcinoma and hypertrophic actinic keratosis, as these are prominent in the infiltrate of discoid lupus erythematosus but are present only as single cells or rare scattered clusters in squamous cell carcinoma and actinic keratosis.[3] Direct immunofluorescence typically shows deposition of immunoglobulins G and M along the basement membrane zone with a frequency similar to typical chronic discoid LE (50–90%), although interpretation must be tempered by the fact that they may be falsely positive when seen in sun-damaged skin.[1] Because hypertrophic lupus erythematosus responds to steroids, some authors suggest that a trial of short course of topical or intralesional steroids may be used to differentiate hypertrophic lupus erythematosus from squamous neoplasia. In addition to multiple keratoacanthomas and squamous cell carcinoma, the differential diagnosis should also include hypertrophic lichen planus, lichenoid drug eruptions, benign lichenoid keratosis, and lichenoid actinic keratosis. Options available for treatment of hypertrophic lupus erythematosus include cryotherapy, topical and intralesional corticosteroids, hydroxychloroquine, isotretinoin, and acitretin.[4],[5]
 |
| Figure 4: Significant improvement after 3 months of acitretin treatment |
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patient has given her consent for his images and other clinical information to be reported in the journal. The patient understand that name and initials will not be published and due efforts will be made to conceal identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
| 1. |
Arps DP, Patel RM. Cutaneous hypertrophic lupus erythematosus: A challenging histopathologic diagnosis in the absence of clinical information. Arch Pathol Lab Med 2013;137:1205-10.
[Google Scholar]
|
| 2. |
Vassallo C, Brazzelli V, Ardigò M, Barbagallo T, Borroni G. Multiple, keratoacanthoma-like nodules on a 47-year-old man: A rare presentation of cutaneous lupus erythematosus. Int J Dermatol 2003;42:950-2.
[Google Scholar]
|
| 3. |
Ko CJ, Srivastava B, Braverman I, Antaya RJ, McNiff JM. Hypertrophic lupus erythematosus: The diagnostic utility of CD123 staining. J Cutan Pathol 2011;38:889-92.
[Google Scholar]
|
| 4. |
Kulkarni S, Kar S, Madke B, Krishnan A, Prasad K. A rare presentation of verrucous/hypertrophic lupus erythematosus: A variant of cutaneous LE. Indian Dermatol Online J 2014;5:87-8.
[Google Scholar]
|
| 5. |
Al-Mutairi N, Rijhwani M, Nour-Eldin O. Hypertrophic lupus erythematosus treated successfully with acitretin as monotherapy. J Dermatol 2005;32:482-6.
[Google Scholar]
|
Fulltext Views
4,110
PDF downloads
2,874





![[Figure - 1]](#fig_ijdvl_2019_85_2_226_229193_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2019_85_2_226_229193_f2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2019_85_2_226_229193_f3.jpg){kind=link}
![[Figure - 4]](#fig_ijdvl_2019_85_2_226_229193_f4.jpg){kind=link}