Translate this page into:
Dome-shaped solitary nodule
Correspondence Address:
Yiqun Jiang
Institute of Dermatology, Chinese Academy of Medical Sciences and Peking Union Medical College, 12, Jiangwangmiao Street, Nanjing 210 042, Jiangsu Province
China
Xiaofang Li
Institute of Dermatology, Chinese Academy of Medical Sciences and Peking Union Medical College, 12, Jiangwangmiao Street, Nanjing 210 042, Jiangsu Province
China
| How to cite this article: Zhang W, He Y, Li X, Jiang Y, Zeng X, Liu W, Sun J. Dome-shaped solitary nodule. Indian J Dermatol Venereol Leprol 2020;86:178-180 |
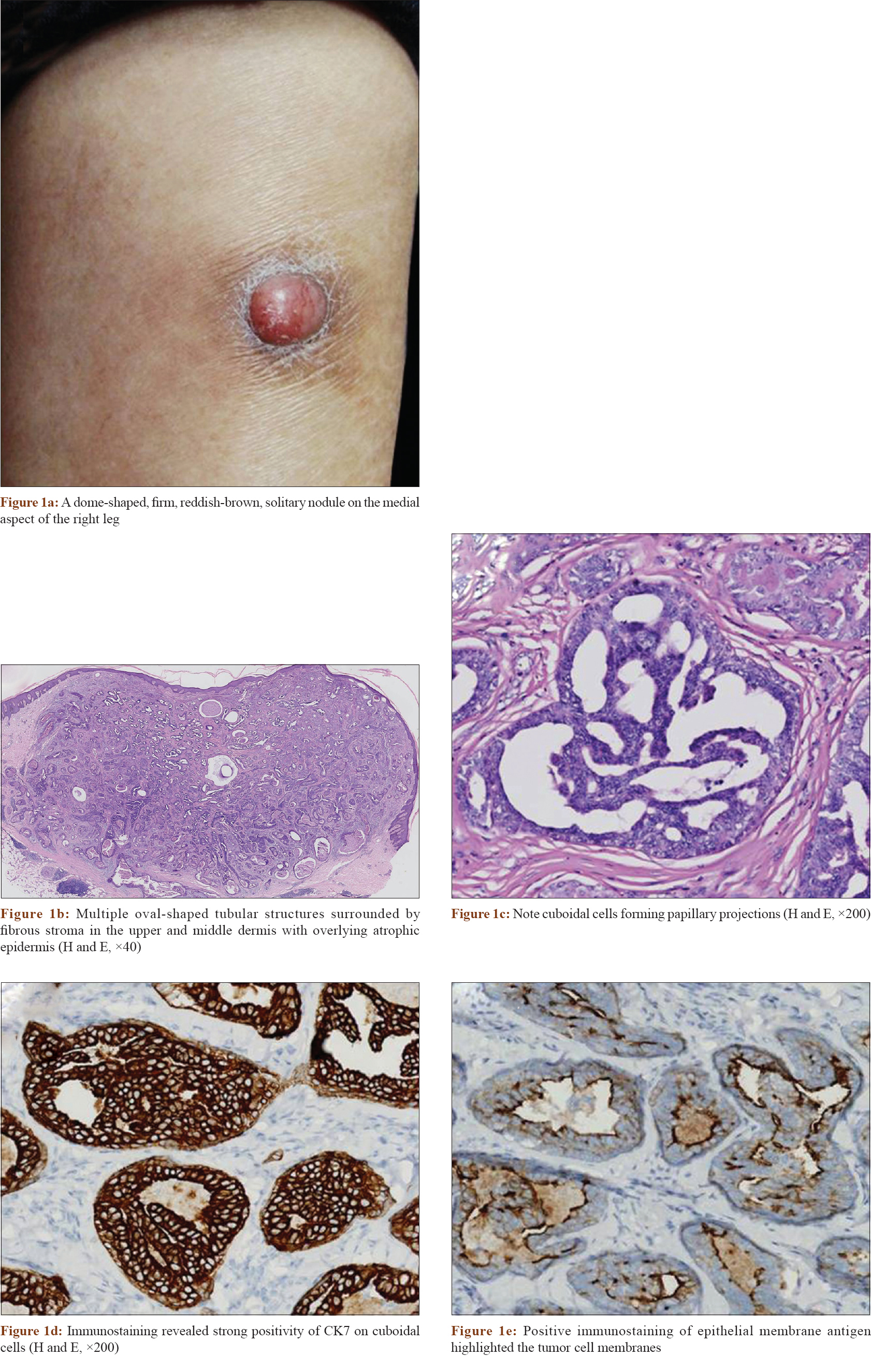
A 64-year-old, otherwise healthy woman was referred to our hospital with a 3-year history of an asymptomatic lesion on the medial aspect of her right leg.
Physical examination disclosed a dome-shaped, firm, reddish-brown, solitary nodule, approximately 3 cm in diameter [Figure - 1]a. She had no previous significant medical or surgical history or a family history of such a tumor. Histopathology showed an unencapsulated, well-circumscribed tumor in the upper to mid dermis. The tumor was composed of multiple, oval to irregularly-shaped, tubular structures lined by two or more layers of epithelial cells and surrounded by fibrous stroma [Figure - 1]b. The luminal layers were composed mainly of cuboidal cells forming papillary projections in some tubules [Figure - 1]c. The peripheral layer was lined with flattened to cuboidal cells. Neither decapitation secretions nor connection of the neoplastic tubules to the overlying epidermis were seen. The overlying epidermis was slightly atrophied. Within some tubules, eosinophilic amorphous material was noted. Cell necrosis, mitosis and nuclear pleomorphism were absent. Immunostaining revealed positivity for cytokeratin-7 [Figure - 1]d. Positive staining with epithelial membrane antigen highlighted the tumor cell membranes [Figure - 1]e. The inner epithelial cells were partly positive for carcinoembryonic antigen. Gross cystic disease fluid protein-15 was negative in tumor cells.
 |
Question
What is the diagnosis?

Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patient has given her consent for her images and other clinical information to be reported in the journal. The patient understands that name and initials will not be published and due efforts will be made to conceal identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
This work was supported by the Fundamental Research Funds for the Central Universities (2016RC320006) and the CAMS Innovation Fund for Medical Sciences (CIFMS-2017-I2M-1-017).
Conflicts of interest
There are no conflicts of interest.
| 1. |
LeBoit PE, Burg G, Weedon D, Sarasin A. World Health Organization Classification of Tumours. Pathology and Genetics of Skin Tumours. Lyon, France: IARC Press; 2006.
[Google Scholar]
|
| 2. |
Blasini W, Hu S, Gugic D, Vincek V. Papillary eccrine adenoma in association with cutaneous horn. Am J Clin Dermatol 2007;8:179-82.
[Google Scholar]
|
| 3. |
Tellechea O, Reis JP, Marques C, Baptista AP. Tubular apocrine adenoma with eccrine and apocrine immunophenotypes or papillary tubular adenoma? Am J Dermatopathol 1995;17:499-505.
[Google Scholar]
|
| 4. |
Mizuoka H, Senzaki H, Shikata N, Uemura Y, Tsubura A. Papillary eccrine adenoma: Immunohistochemical study and literature review. J Cutan Pathol 1998;25:59-64.
[Google Scholar]
|
| 5. |
Ichikawa E, Okabe S, Umebayashi Y, Iijima S, Otsuka F, Watanabe S, et al. Papillary eccrine adenoma: Immunohistochemical studies of keratin expression. J Cutan Pathol 1997;24:564-70.
[Google Scholar]
|
Fulltext Views
3,931
PDF downloads
4,256





![[Figure - 1]](#fig_ijdvl_2020_86_2_178_241562_f1.jpg){kind=link}