Translate this page into:
Epidermal nuclear staining: A distinct reaction pattern in connective tissue diseases
Correspondence Address:
Raghavendra Rao
Department of Skin and V.D, Kasturba Medical College, Manipal - 576 104, Karnataka
India
| How to cite this article: Rao R, Balachandran C. Epidermal nuclear staining: A distinct reaction pattern in connective tissue diseases. Indian J Dermatol Venereol Leprol 2007;73:120-121 |
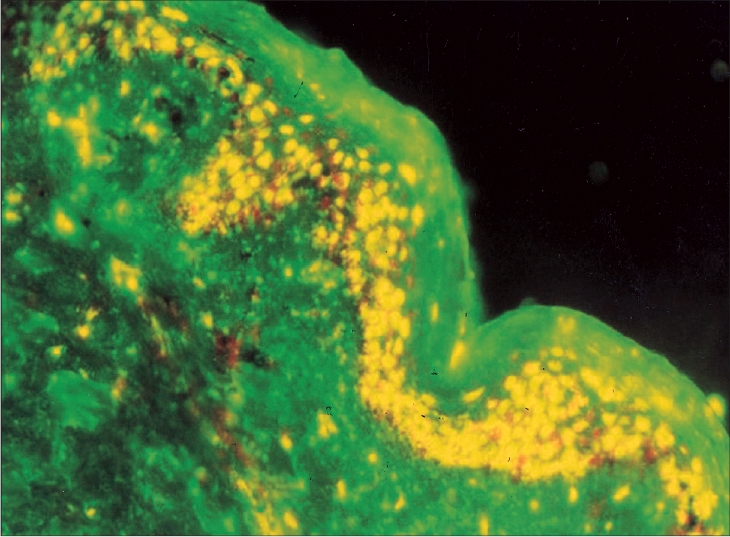 |
| IgG epidermal nuclear staining (DIF, x200) |
|
| IgG epidermal nuclear staining (DIF, x200) |
Sir,
Role of direct immunofluorescence (DIF) in the diagnosis of lupus erythematosus (LE) and other connective tissue diseases (CTD) is well-established. Deposition of various immunoreactants along the dermal-epidermal junction (DEJ) is highly characteristic of LE. However, DEJ is not the only site of immunopathological changes in connective tissue diseases. Immunoreactants may also be deposited in the epidermis (seen as epidermal nuclear staining or ENS) or in the papillary dermis. [1] Our objective was to study the prevalence of ENS in various connective tissue diseases and to find out if there was any association between ENS and serological abnormalities.
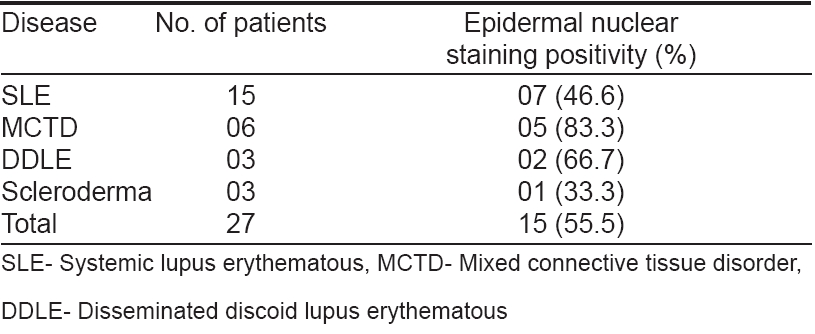
Twenty-seven patients (2 males and 25 females with a mean age of 27.9 years) attending skin OPD between January- December 2005 with a clinical diagnosis of CTDs were included in the study. Diagnostic distribution of patients is tabulated [Table - 1]. Punch biopsies (each measuring 3.5 mm in size) were taken from the lesional skin, sun-exposed non-lesional and covered gluteal skin and subjected to direct immunofluorescence test. A retrospective analysis of serological abnormalities was done in each case.
We could demonstrate ENS with IgG class of antibody in total 15 (55.5%) of our patients [Figure - 1]. It was seen most commonly in patients with MCTD (5/6 patients; 83.3%) followed by DDLE and SLE patients (66.7% and 46.6% respectively). ENS was observed both in lesional and non-lesional (sun-exposed as well as covered) skin. Lupus- band test (LBT) was positive in 14/15 patients. Most common serological abnormalities detected in our patients with a positive ENS were antibodies to ribonucleoprotein (anti-RNP, 8 patients) and anti-Sm antibodies (7 patients) followed by anti-dsDNA in 4 patients and anti-Scl-70 in 2 patients.
Epidermal nuclear staining occurs as a result of anti-nuclear antibody (ANA) deposition in the nucleus of keratinocyte (′ In vivo ANA′). The frequency with which it occurs in various CTD′s varies between 2.6-9.8%. [2] The high prevalence in our study could be due to the smaller study sample. Four different patterns of ENS (viz. speckled, homogenous, nucleolar and rim) have been reported in the literature with speckled pattern being the commonest type. The patterns of ENS in the skin correlate with that of serum ANA in majority of cases. [3] The pattern of staining was not recorded in our study. Rodrigues et al found no association between this phenomenon and LBT. [4] Deposition of immunoglobulin does not cause any pathological changes per se , as it has been observed in both lesional skin and normal skin. In addition to skin, it has also been demonstrated in the renal and pulmonary tissues. [5] Though we found the occurrence of ENS with only IgG class of antibodies, others have described ENS with IgM and IgA classes also. [6]
There exists a strong association between serum antibodies to saline-soluble (extractable) nuclear antigen (ENA) and speckled pattern of immunoglobulin localization in epidermal nuclei. ENA contains ribonuclease sensitive (ribonucleoprotein or RNP) and ribonuclease resistant (Sm antigen) component. [7] It is a well-established fact that high titre of anti-RNP antibodies is commonly found in patients with MCTD. Consequently, ENS was found most commonly in our patients with MCTD.
Gilliam suggested that ENS was an in vitro phenomenon occurring as a result of contamination of epidermal nuclei by diffusible ANA in the dermis during the processing of specimen. [8] This was later contradicted by Izuno who proved that ENS is a true in vivo process. Further, he speculated that serum of these patients contains permeability enhancing factor, which increases the permeation of antibodies across the dermal-epidermal junction. [9]
Demonstration of ENS by DIF may have certain important clinical implications. It may be an indicator of less aggressive form of CTD as these patients will have a low incidence of renal damage. [10] On the other hand, a high incidence of oral ulceration and Raynaud′s phenomenon have been reported. [2],[11]
To conclude ENS is a distinct marker, the presence of which corroborates the diagnosis of connective tissue diseases.
| 1. |
Vassileva S. Lupus erythematosus. In: Kanitakis J, Vassileva S, Woodley D, editors. Diagnostic immunohistochemistry of the skin. 1 st ed. Chapman-Hall: London; 1998. p. 144-52.
[Google Scholar]
|
| 2. |
Burrows NP, Bhogal BS, Russel Jones R, Black MM. Clinicopathological significance of cutaneous epidermal nuclear staining by direct immunofluorescence. J Cutan Pathol 1993;20:159-62.
[Google Scholar]
|
| 3. |
Kallenberg CG, de Jong MC, Walstra TM, Kardaun S, The TH. In vivo antinuclear antibodies (ANA) in biopsies of normal skin: Diagnostic significance and relation to serum ANA. J Rheumatol 1983;10:733-40.
[Google Scholar]
|
| 4. |
Rodriguez CJ, de Oliveira RM, Taniwaki NN, Bueno C, Marchiori P, Cossermelli W. Epidermal nuclear immunoglobulin deposition in connective tissue diseases. Rev Hosp Clin Fac Med Sao Paulo 1990;45:154-7.
[Google Scholar]
|
| 5. |
Williams WV, Barjenbrach P, Adelstein E, Sharp GC, Walker SE. The clinical significance of the in vivo antinuclear antibody phenomenon. Arch Pathol Lab Med 1986;110:798-802.
[Google Scholar]
|
| 6. |
Velthuis PJ, Kater L, van der Tweel L, Meyling FG, Derksen RH, Hene RJ, et al . In vivo antinuclear antibody of the skin. Diagnostic significance and association with selective antinuclear antibodies. Ann Rheum Dis 1990;49:163-7.
[Google Scholar]
|
| 7. |
Gilliam JN, Prystowsky SD. Mixed connective tissue diseases syndrome. Arch Dermatol 1977;113:583-7.
[Google Scholar]
|
| 8. |
Gilliam JN. The significance of cutaneous immunoglobulin deposits in lupus erythematosus and NZB/NZW F1 hybrid mice. J Invest Dermatol 1975;65:154-61.
[Google Scholar]
|
| 9. |
Izuno GT. Observations on the in vivo reaction of antinuclear antibodies with epidermal cells. Br J Dermatol 1978;98:391-8.
[Google Scholar]
|
| 10. |
Bukilica MN, Andrejevic SB, Bonaci-Nikolic BM, Nikolic MM. Speckled antinuclear antibodies in keratinocytes- what does it mean? Clin Exp Rheumatol 2002;20:499-504.
[Google Scholar]
|
| 11. |
Prystowsky SD, Tuffanelli DL. Speckled (particulate) epidermal nuclear IgG deposition in normal skin. Correlation of clinical features and laboratory findings in 46 patients with a subset of connective tissue disease characterized by antibody to extractable nuclear antigen. Arch Dermatol 1978;114:705-10.
[Google Scholar]
|
Fulltext Views
2,832
PDF downloads
1,727





![[Table - 1]](#tbl_ijdvl_2007_73_2_120_31901_2.jpg){kind=link}
![[Figure - 1]](#fig_ijdvl_2007_73_2_120_31901_1.jpg){kind=link}