Translate this page into:
Epidermoid cyst of penis
2 Department of Dermatology, Guru Gobind Singh Medical College and Hospital, Faridkot, Punjab, India
Correspondence Address:
Sumitoj Singh
48, Medical college campus, Faridkot, Punjab
India
| How to cite this article: Singh S, Kaur T. Epidermoid cyst of penis. Indian J Dermatol Venereol Leprol 2011;77:627 |
Sir,
A 33-year-old male presented with swelling on penis since 2 years. It was painless and slowly increasing in size. There was no history of local trauma or infection. Physical examination revealed smooth, soft, painless cystic swelling, 2.5 cm in diameter on the ventrolateral surface of the shaft of penis, about 3 cm from the glans [Figure - 1]. The lesion was excised surgically under local anesthesia and there was no communication with the urethra. On cut section, it contained cheesy material and histopathological examination showed cyst lined by stratified squamous epithelium and did not contain skin appendages or derivatives of other germ cells [Figure - 2].
 |
| Figure 1: Epidermoid cyst on ventrolateral surface of penis |
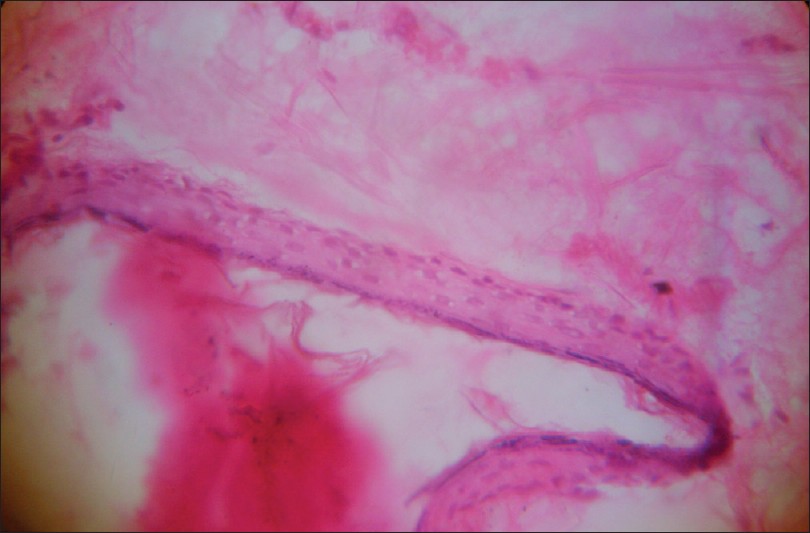 |
| Figure 2: Histopathology showing cyst lined with stratified squamous epithelium (H and E, ×200) |
Epidermoid cysts represent the most common cutaneous cysts. They can occur anywhere on the body, and the most frequent sites involved are face, scalp, neck, and trunk. Penile epidermoid cysts are uncommon, and only few cases have been reported in the literature. [1] The exact etiology of penile epidermoid cyst is not clear. It can be congenital or acquired. Acquired cyst of the penis is either due to trauma or occurs after surgery. Some authors have suggested that it may originate from a median raphe cyst and others have suggested that median raphe cyst is a different entity from epidermoid cyst. [2]
Median raphe cyst develops anywhere in midline along the penoscrotal raphe from urethral meatus to anus, usually in the distal area near glans penis. Median raphe cyst arises due to defects in embryological development of the male genitalia. They develop from urethral and epithelium remains, incidental to incomplete closure of genital folds, or from split off growths of embryological epithelium after primary closure of the folds. [3] Epithelial lining of the median raphe cyst corresponds to that part of urethra from which it originates, stratified squamous epithelium in the distal portion (ectodermal origin) and pseudo-stratified columnar epithelium when it originates from the rest of the urethra (endodermal origin). Three histological types have been described: (1) urethral type (70%) with epithelium similar to the urethra; (2) epidermoid type (10%) composed of squamous epithelium; and (3) mixed type formed by a combination of the above. Immunostaining with cytokeratin 7 can confirm urothelial origin of median raphe cyst as it is a marker of urothelial epithelium and absent in stratified epithelium of skin. [3] In present case, cyst is more likely to be true epidermoid cyst and not median raphe cyst as it was not in the midline on the genitoperineal raphe.
Other differential diagnosis of penile epidermoid cysts includes extensive range of conditions, e.g.., dermoid cysts, pilonidal cysts, teratoma, and urethral diverticula. [4],[5] The dermoid cyst differs from epidermoid cyst only in the presence within its walls of normal or dysmorphic adnexal appendages, usually sebaceous glands or abortive hair follicles. Teratoma contains derivatives from other germ cells such as muscle or bone. Unlike urethral diverticulum, epidermoid cyst does not communicate with the urethra.
The indications for treatment of these cysts are secondary infection, urinary tract obstruction, pain on intercourse, and cosmetic reason. In our case, excision was done for cosmetic reason. The best treatment option is total excision. Neoplastic change very rarely develops in epidermoid cysts at other sites, but no reports of malignant change in penile epidermoid cysts have been reported so far. [1],[5]
| 1. |
Suwa M, Takeda M, Bilim V, Takahashi K. Epidermoid cyst of the penis: A case report and review of the literature. Int J Urol 2000;7:431-3.
[Google Scholar]
|
| 2. |
Little JS Jr, Keating MA, Rink RC. Median raphe cysts of the genitalia. J Urol 1992;148:1872-3.
[Google Scholar]
|
| 3. |
Navarro HP, Lopez PC, Ruiz JM, Martinez Sanchiz C, Cha SH, Sanchez AS, et al. Median raphe cyst. Report of two cases and literature review. Arch Esp Urol 2009;62:585-9.
[Google Scholar]
|
| 4. |
Rattan J, Rattan S, Gupta DK. Epidermoid cyst of the penis with extension into the pelvis. J Urol 1997;158:593.
[Google Scholar]
|
| 5. |
Unsal A, Cimentepe E, Saglam R. Penile epidermoid cyst in an elderly patient. Int Urol Nephrol 2002;34:229-30.
[Google Scholar]
|
Fulltext Views
12,237
PDF downloads
1,733





![[Figure - 1]](#fig_ijdvl_2011_77_5_627_84085_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2011_77_5_627_84085_f2.jpg){kind=link}