Translate this page into:
Epithelioid blue nevus not associated with Carney complex in a Korean patient
Correspondence Address:
Kee Suck Suh
Department of Dermatology, Kosin University College of Medicine, 34 Amnam-Dong, Seo-gu, Busan, 602-702
South Korea
| How to cite this article: Jang MS, Kang DY, Park JB, Kim ST, Suh KS. Epithelioid blue nevus not associated with Carney complex in a Korean patient. Indian J Dermatol Venereol Leprol 2012;78:521 |
Sir,
Epithelioid blue nevus (EBN) is a distinctive variant of blue nevus. EBN is important because of its strong association with the Carney complex (myxomas, spotty skin pigmentation, endocrine overactivity, psammomatous melanotic schwannomas), which is inherited in an autosomal dominant manner. [1] However, sporadic EBN has rarely been reported in Asians.
A 36-year-old Korean woman presented with a 30-year history of an asymptomatic pigmented nodule on the right shin. Physical examination revealed a dome-shaped, blue-black nodule that was 1.0 cm in diameter [Figure - 1]. The lesion was well-circumscribed and firm on palpation. Excisional biopsy was performed with a presumed diagnosis of blue nevus. Histopathologic findings showed a well-demarcated, heavily pigmented, wedge-shaped, dermal tumor, separated by a thin band of uninvolved dermis from the epidermis [Figure - 2]a. The majority of the specimen was made up of medium to large pigmented cells that were globular and polygonal (epithelioid), and a minority of cells that were spindled and dendritic. Epithelioid melanocytes and melanophages were diffusely intermixed with a variable number of collagen bundles [Figure - 2]b.
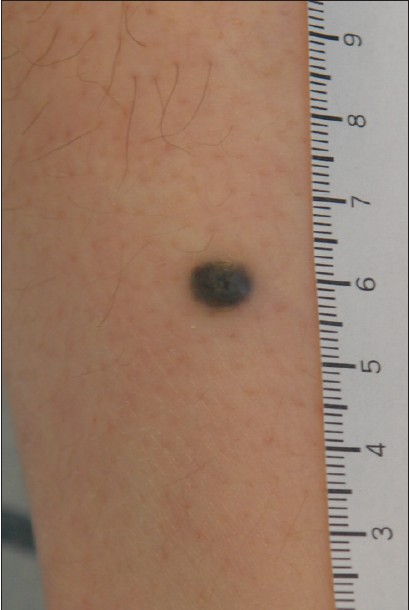 |
| Figure 1: Solitary asymptomatic blue-black, bean-sized, elevated, dome-shaped nodule on the right shin. |
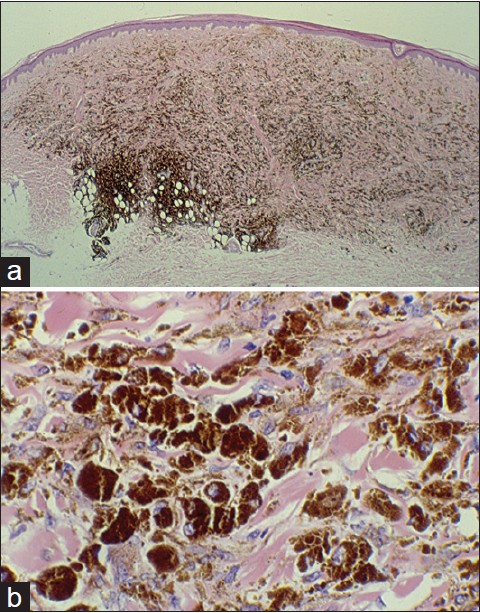 |
| Figure 2: (a) The domed, relatively well-demarcated, wedge-shaped, heavily pigmented proliferation extended from the papillary dermis through the deep reticular dermis and focally approached the subcutis (H and E, ×20). (b) The heavily melanin-laden globular, epithelioid melanocytes and melanin-containing macrophages were dispersed among collagen bundles in the reticular dermis (H and E, ×200) |
No part of the lesion showed junctional activity, fibrosis, necrosis, atypical cell and mitotic figures. The results of immunohistochemical staining showed positive S-100 and CD 68 staining, focally positive HMB-45 staining, and negative Ki-67 staining [Figure - 3]a, b. A diagnosis of EBN was made based on clinical and histopathological findings. The patient had no family history of similar lesions or of Carney complex. Hormonal studies, echocardiography and meticulous skin examinations were performed to rule out Carney complex, and the results were unremarkable. No evidence of recurrence was observed for a period of 8 months.
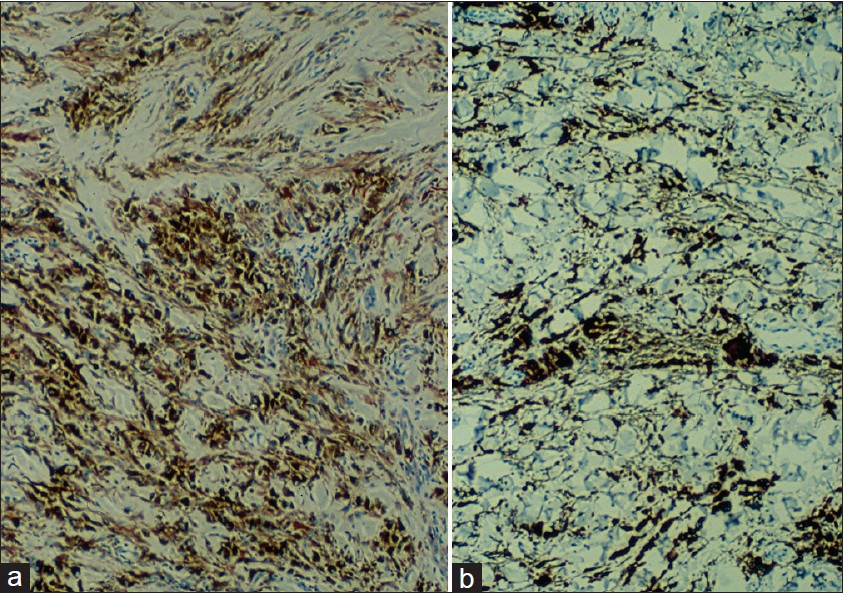 |
| Figure 3: (a) Epithelioid melanocytes stained positive for S-100 (×200). (b) Positive stain for CD-68 (×200). |
EBN mainly presents as solitary, heavily pigmented, blue-black, dome-shaped nodules, or less commonly, as multiple nodules. [2] Histopathologically, EBN is entirely intradermal melanocytic nevi, composing mostly of heavy pigmented epithelioid cells and consisting of 2 types of melanocytes with non-nested features: one intensely pigmented, globular and fusiform melanocytes: and the other less pigmented melanocytes with polygonal and large cytoplasm. [1] In some cells, an accentuation of the pigment contents is only seen at the periphery of the cytoplasm without pigmentation around nucleus, showing ′egg-fried′ appearance. [2]
The clinico-pathologic differential diagnosis for EBN includes malignant melanoma, Spitz nevus, malignant blue nevus and animal type melanoma. [1],[3],[4],[5]
Malignant melanoma is clinically characterized by asymmetry, border irregularity, color variegation and large diameter (greater than 6 mm). Histopathologically, malignant melanoma typically shows junctional activity, epidermal invasion, infiltrating margins, peripheral inflammation, abundant and atypical mitoses, cytologic atypia and tissue necrosis. These findings are usually not seen in EBN. [4]
Spitz nevi are composed of spindled cells, epithelioid cells or a mixture of both. This entity is characteristically sparsely pigmented, tends to be located in the reticular dermis, and the featured cells are in nests. Moreover, dull pink globules (Kamino bodies) can be seen in the dermo-epidermal junction. In contrast, EBN is deeply pigmented, typically stretches from the papillary dermis to the subcutis, and shows an interstitial growth pattern of its cells.
Among the variants of Spitz nevus, pigmented epithelioid cell nevus (PECN) is a more problematic entity in the differential diagnosis of EBN because both EBN and PECN may be composed of intensely pigmented, epithelioid and spindled melanocytes. [1],[3] However, compared to PECN, EBN usually lacks a junctional melanocytic component, and dermal dendritic melanocytes are typically found intermingled with intensely pigmented epithelioid melanocytes, demonstrating a small basophilic nucleus. [3]
In contrast to EBN, malignant blue nevus (MBN) typically shows significant nuclear pleomorphism, hyperchromasia, prominent eosinophilic nucleoli, necrosis, and brisk mitotic activity. An increased proliferative activity can be also identified by analysis of Ki-67 staining. [4]
Pigment synthesizing melanoma (so-called animal type melanoma, PSM) is composed of a mixture of epithelioid and spindled melanocytes with heavy pigmentation, and its appearance closely resembles EBN. However, cytological atypia, mitotic activity and epidermal involvement favor more the diagnosis of PSM. In addition, melanocytes with epithelioid morphology are more prominent in EBN while in PSM, there is a mixture of epithelioid and short spindle-shaped melanocytes. Clinically, PSM can also be distinguished from EBN by the occasional predominance of ulceration, regional lymph node metastases, recurrences and systemic involvement. [5]
Not all EBN are associated with the Carney complex, but if EBN are found, it is important to be aware of potential comorbid diseases that are parts of the Carney complex. It is also important in the differential diagnosis for malignant melanoma and other melanocytic lesions to accurately recognize histopathologic features of EBN.
| 1. |
Carney JA, Ferreiro JA. The epithelioid blue nevus. A multicentric familial tumor with important associations, including cardiac myxoma and psammomatous melanotic schwannoma. Am J Surg Pathol 1996;20:259-72.
[Google Scholar]
|
| 2. |
Pinto A, Raghavendra S, Lee R, DeRossi S, Alawi F. Epithelioid blue nevus of the oral mucosa: A rare histologic variant. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2003;96:429-36.
[Google Scholar]
|
| 3. |
Luzur B, Bastian BC, Calonje E. Melanocytic nevi. In: McKee PH, editor. McKee's pathology of the skin with clinical correlations. 4 th ed. Boston: Saunders; 2011. p. 1150-220.
th ed. Boston: Saunders; 2011. p. 1150-220.'>[Google Scholar]
|
| 4. |
Martin RC, Murali R, Scolyer RA, Fitzgerald P, Colman MH, Thompson JF. So-called "malignant blue nevus": A clinicopathologic study of 23 patients. Cancer 2009;115: 2949-55.
[Google Scholar]
|
| 5. |
Ludgate MW, Fullen DR, Lee J, Rees R, Sabel MS, Wong SL, et al. Animal-type melanoma: A clinical and histopathological study of 22 cases from a single institution. Br J Dermatol 2010;162:129-36.
[Google Scholar]
|
Fulltext Views
3,685
PDF downloads
1,803





![[Figure - 1]](#fig_ijdvl_2012_78_4_521_98105_u1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2012_78_4_521_98105_u2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2012_78_4_521_98105_u3.jpg){kind=link}