Translate this page into:
Eruptive collagenoma
2 Department of Pathology, University College of Medical Sciences (University of Delhi) and Guru Teg Bahadur Hospital, Delhi, India
Correspondence Address:
Reena Sharma
C-304, Shri Sai Baba Apartment, Sector- 9, Rohini, Delhi - 110 085
India
| How to cite this article: Sharma R, Verma P, Singal A, Sharma S. Eruptive collagenoma. Indian J Dermatol Venereol Leprol 2013;79:256-258 |
Sir,
Collagenoma is a connective tissue nevus, a hamartoma, the pathogenesis of which is elusive. The major element of the extracellular connective tissue within a connective tissue nevus may be collagen, elastic fibers or glycosaminoglycans. [1] Eruptive collagenoma is a rare type of collagenoma that was first reported and named by Colomb in 1955. [2] Herein, a case of eruptive collagenoma along with review of the literature has been presented.
A 14-year-old girl presented to us with sudden-onset eruption of asymptomatic skin-colored papules over the back and neck within a period of 3-4 days, 4 months back. There was no history of previous skin eruptions/chicken pox or trauma at the site of the lesions. Her family history was unremarkable. A review of the various organ systems (cardiovascular, respiratory, gastrointestinal tract, central nervous system) was within normal limits. Examination revealed multiple discrete, firm, non-tender skin-colored to slightly hypopigmented papules, 2-5 mm in diameter, which had no scale or exudation on the surface [Figure - 1]. The lesions were present predominantly over the lower back, with a few scattered lesions over the chest and upper thighs. Clinical differential diagnosis of steatocystoma multiplex, eruptive xanthoma, anetoderma, papular elastorrhexis and eruptive collagenoma were kept.
 |
| Figure 1: Multiple discrete, 2-5 mm in diameter, firm, non-tender skin-colored to slightly hypopigmented papules over the lower back |
There was no evidence of osteopoikilosis or any other bony abnormality on radiographic examination of the hands and pelvic bones. The hematological and biochemical investigations including complete blood counts (CBC), liver and kidney function tests and electrocardiogram (ECG) were normal. Histopathological examination of the section from a representative lesion revealed an unremarkable epidermis. The reticular dermis was expanded by randomly arranged coarse collagen bundles of various sizes [Figure - 2]. Verhoff Van Gieson stain revealed markedly decreased elastic fibers in the dermis [Figure - 3]. Based on these findings, the patient was diagnosed as having eruptive collagenoma.
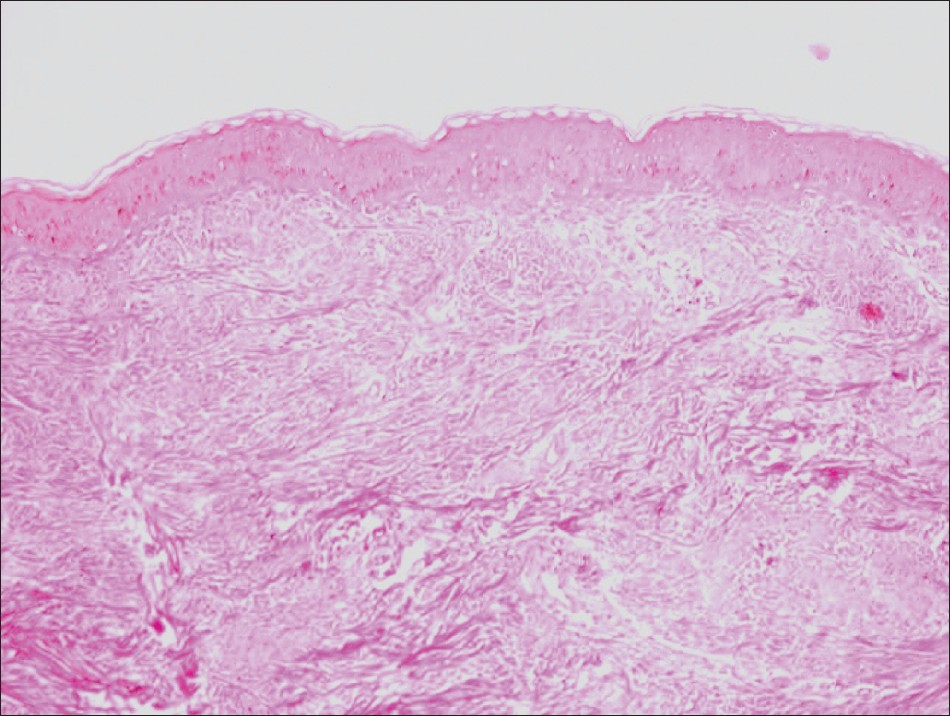 |
| Figure 2: Randomly arranged bundles of collagen fibers present throughout the dermis (H and E, × 400) |
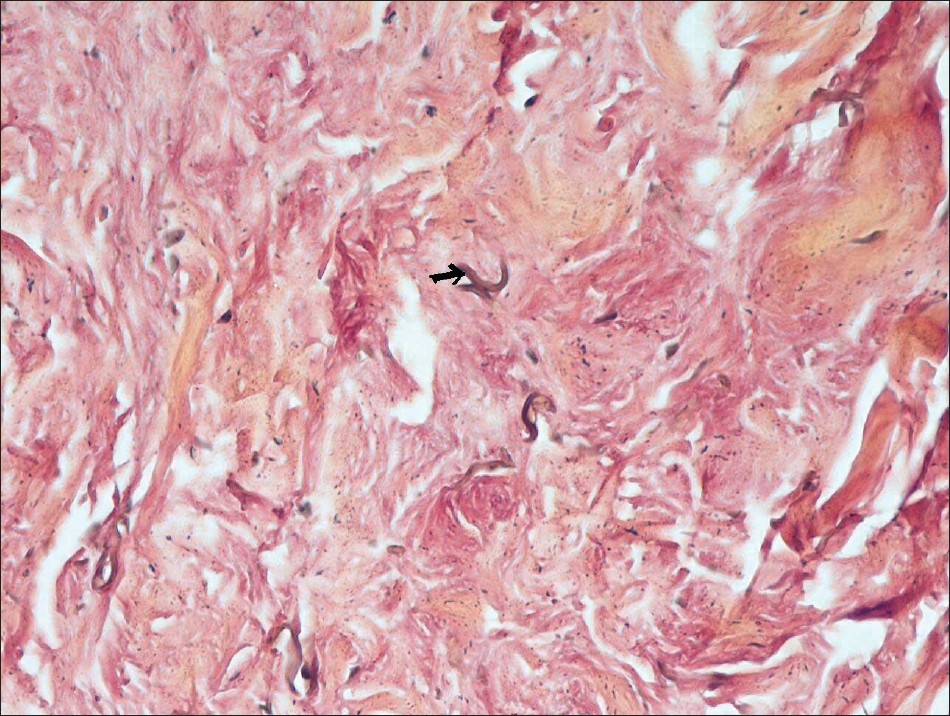 |
| Figure 3: Markedly decreased elastic fibers in the dermis as depicted by an arrow (Verhoff-Van Geison stain, × 400) |
Collagenomas are divided into inherited and acquired. The former, which are autosomal dominantly inherited, include familial cutaneous collagenoma and Shagreen patch of tuberous sclerosis; the latter include eruptive collagenoma and isolated collagenoma. [3] Acquired collagenomas may be multiple when they are termed eruptive collagenoma, or they may be isolated and localized to one body region only. [3] Familial cutaneous collagenomas usually appear in the second and third decades of life, while eruptive collagenomas, like isolated collagenomas, may appear within a few years after birth. [4] However, eruptive collagenomas have also been reported in the later years of life. [5],[6] Familial cutaneous collagenomas tend to affect the trunk (mostly the upper back) and proximal arms, whereas eruptive collagenomas usually affect the periphery, including the head, neck and upper and lower limbs, although cases affecting the trunk as in the present case have been reported. [4] Lesions are usually symmetrical in both familial and eruptive variety, but are more numerous (even in hundreds) in familial cutaneous collagenomas as compared with the eruptive collagenomas. Isolated collagenomas present as few lesions localized to parts of the body such as palm, sole and labium majus. [3] Our case fits into eruptive rather than the familial variety because of the negative family history. Eruptive cutaneous collagenoma is clinically characterized by discrete, firm, skin-colored and slightly elevated cutaneous papules, nodules or plaques on the trunk and the extremities, or it may be generalized. [5] Histologically, the lesions are characterized by an excessive accumulation of dense, coarse collagen fibers in the dermis. Elastic fibers appear diminished in number, perhaps representing a dilution phenomenon due to excess collagen accumulation. [4]
Elastic nevus, nevus anelasticus and papular elastorrhexis, scars and anetoderma are the differential diagnosis of eruptive collagenoma. Elastic nevus can occur as solitary lesion or associated with osteopoikilosis of Buschke Ollendorf syndrome. [7] Biopsy is required to make the diagnosis. Nevus anelasticus has been defined as an acquired nevus characterized clinically by perifollicular lesions and histopathological evidence of paucity or lack of elastic tissue, while collagen is normal. [8] Besides, papular elastorrhexis is another condition characterized by asymptomatic, smaller 1-5 mm- sized, white papules on the trunk and extremities first appearing during childhood or adolescence. [8] Histopathologically, papular elastorrhexis displays fragmented elastic fibers unlike eruptive collagenoma, where elastic fibers appear diminished rather than fragmented. [8]
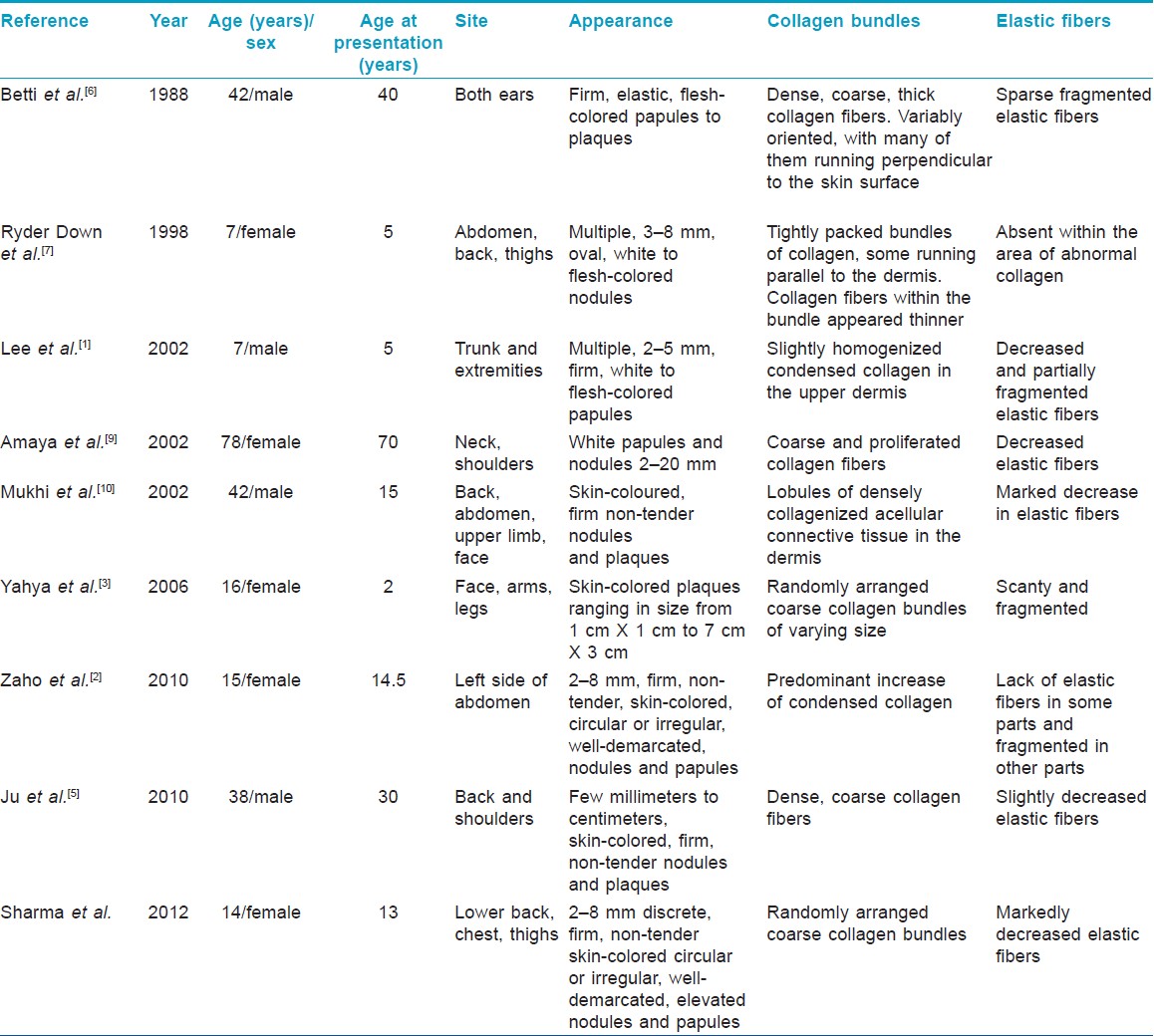
To the best of our knowledge, only eight reported cases of eruptive collagenoma could be retrieved in the English literature by searching on PUBMED/MEDLINE, the salient features of which have been outlined in [Table - 1].
Because the lesions are benign, no active intervention is required. It is imperative to take cognizance of eruptive collagenoma as it may masquerade as a number of dermatosis. A histopathological study comprising stains for connective tissue is essential in order to reach the precise diagnosis. [10]
| 1. |
Lee MW, Choi JH, Sung KJ, Moon KC, Koh JK. A case of eruptive collagenoma. Pediatr Dermatol 2002;19:565-7.
[Google Scholar]
|
| 2. |
Zhao C, Ma W, Wang Y, Sun Q. Female with eruptive collagenoma clustered in the left lateral aspect of the abdomen. J Dermatol 2010;37:843-5.
[Google Scholar]
|
| 3. |
Yahya H, Rafindadi AH. Eruptive collagenoma in a Nigerian girl. Int J Dermatol 2006;45:1344-6.
[Google Scholar]
|
| 4. |
Uitto J, Santa Cruz DJ, Eisen AZ. Familial cutaneous collagenoma: Genetic studies on a family. Br J Dermatol 1979;101:185-95.
[Google Scholar]
|
| 5. |
Ju Q, Song N, Sun J. Eruptive cutaneous collagenoma in a Chinese patient. J Dermatol 2011;38:399-401.
[Google Scholar]
|
| 6. |
Betti R, Inselvini E, Pazzini C, Moneghini L, Crosti C. Symmetrical, papular, eruptive auricular collagenomas. J Am Acad Dermatol 1988;39:363-4.
[Google Scholar]
|
| 7. |
Ryder Down AM, Lear JT, Condon CA, Porter H, Kennedy CT.Eruptive collagenomas of the skin: A case history. Pediatr Dermatol 1998;4:269-70.
[Google Scholar]
|
| 8. |
Ryder HF, Antaya RJ. Nevus anelasticus, papular elastorrhexis, and eruptive collagenoma: Clinically similar entities with focal absence of elastic fibers in childhood. Pediatr Dermatol 2005;22:153-7.
[Google Scholar]
|
| 9. |
Amaya M, Okubo Y, Koga M. A case of eruptive collagenoma localized on the neck and shoulders. J Dermatol 2002;29:79-85.
[Google Scholar]
|
| 10. |
Mukhi SV, Kumar P, Yuvarajkumar D, Raghuveer CV. Eruptive collagenoma. Indian J Dermatol Venereol Leprol 2002;68:98-9.
[Google Scholar]
|
Fulltext Views
9,199
PDF downloads
1,635





![[Figure - 1]](#fig_ijdvl_2013_79_2_256_107658_f2.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2013_79_2_256_107658_f3.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2013_79_2_256_107658_f4.jpg){kind=link}
![[Table - 1]](#tbl_ijdvl_2013_79_2_256_107658_t1.jpg){kind=link}