Translate this page into:
Erythematous eroded plaque on the left nipple in a 75-year-old woman
2 Department of Pathology, Faculty of Medicine, Pontificia Universidad Católica De Chile, Santiago, Chile
Correspondence Address:
Sergio González-Bombardiére
Vicuña Mackenna 4686, Macul, Santiago
Chile
| How to cite this article: Alvarez-Veliz S, Majluf-Caceres P, González-Bombardiére S. Erythematous eroded plaque on the left nipple in a 75-year-old woman. Indian J Dermatol Venereol Leprol 2019;85:307-309 |
A 75-year-old woman presented with a 2-year history of a painful, ulcerated lesion on the left nipple, with intermittent bloody discharge. Physical examination revealed an erythematous eroded plaque on the left areola and nipple [Figure - 1]. Dermoscopy showed a pink structureless zone, ulceration with sticky-fiber sign (hair fibers trapped in the crust of the ulcer) and cherry red spots [Figure - 2]. Mammographic echography and mammography had no signs of malignancy.
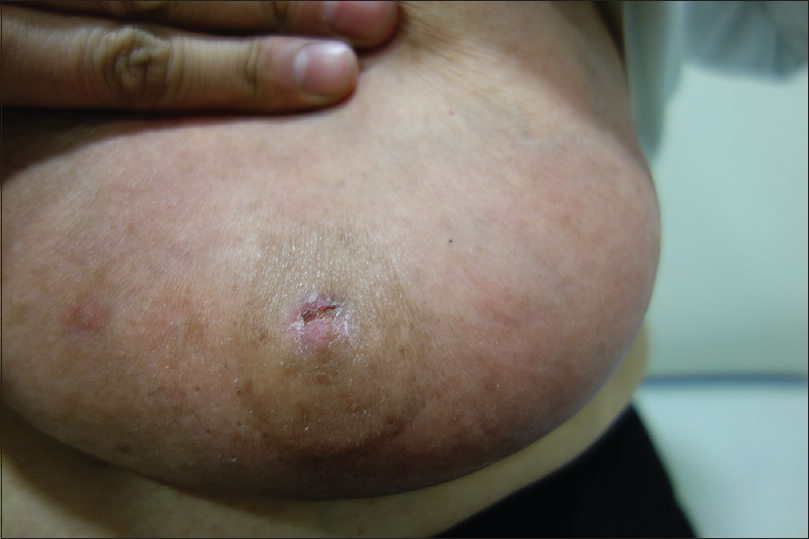 |
| Figure 1: Erythematous eroded plaque on the left areola and nipple |
 |
| Figure 2: Dermoscopy showed a pink structureless zone, ulceration (green arrow) with fiber sign (black arrow) and cherry red spots (blue arrow) |
A biopsy was performed from the plaque for histological examination. Hematoxylin and eosin (H and E) staining of the biopsy revealed an ulcerated, well-circumscribed proliferation of tubular glands [Figure - 3]a, with some luminal papillary projections [Figure - 3]b. Two rows of normotypic epithelial cells and discrete stromal lymphoplasmocellular inflammation were also seen; decapitation of luminal cells was evident and basal myoepithelial cells were also visible [Figure - 3]c. No necrosis, atypical mitoses or cellular pleomorphism were observed.
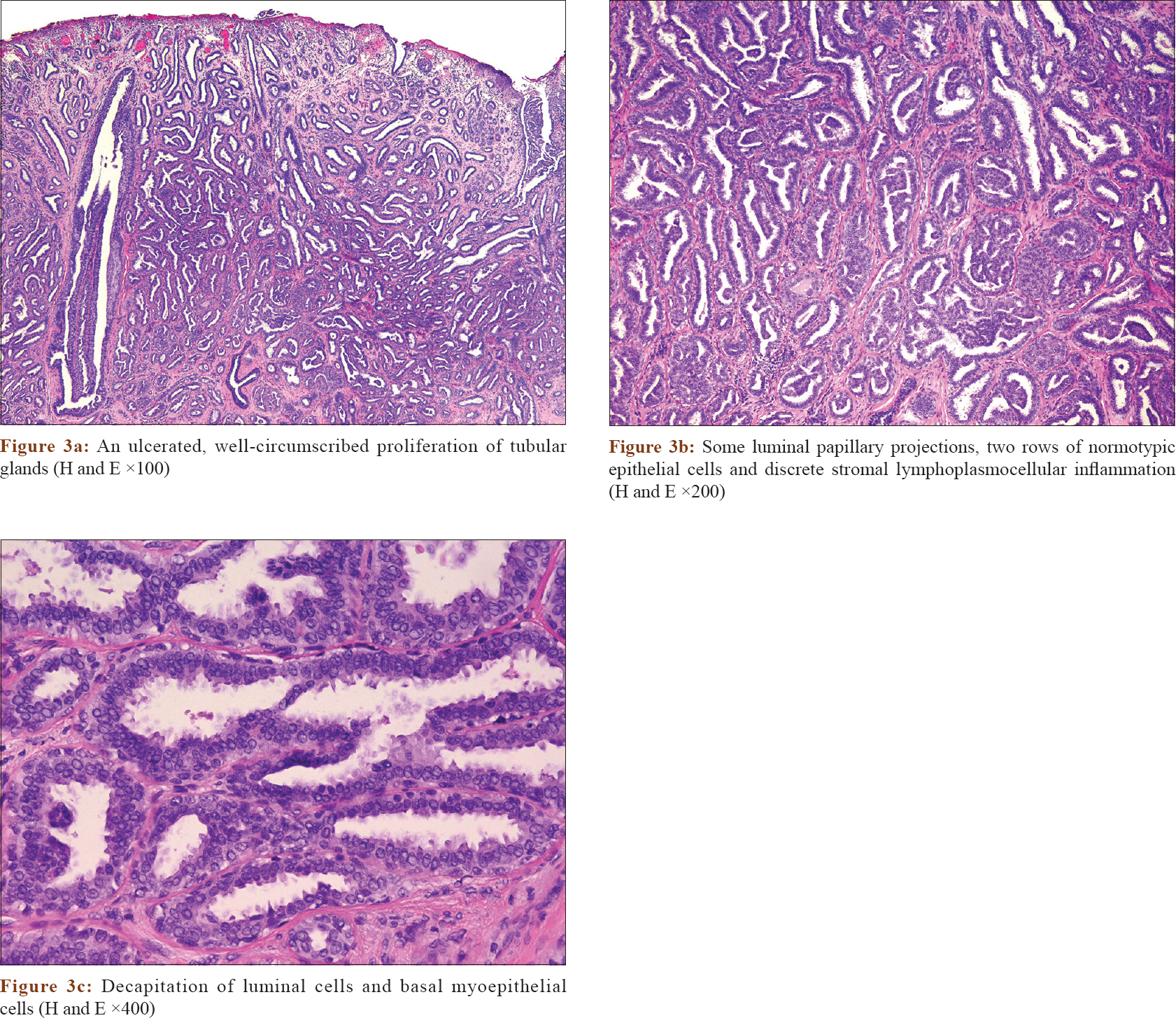 |
| Figure 3: |
Question
What is your diagnosis?
Answer
Erosive adenomatosis of the nipple.
Review
Erosive adenomatosis of the nipple or florid papillomatosis of nipple, is an uncommon and under-recognized pathology of the breast. It is a benign proliferative neoplasm of lactiferous ducts of the nipple, seen predominantly in middle-aged women, but also reported in men and children.[1] It is clinically polymorphic and presents as erythema, nodule or erosion, usually unilateral. The serous or sanguineous discharge from the surface of the nipple is commonly reported as an initial presenting symptomatology. In contrast to mammary Paget's disease in which it is a genuine nipple discharge, in erosive adenomatosis of the nipple it is secondary to the presence of an erosive lesion on the nipple. It has been reported that patients consult years after the onset of the first symptoms.[1]
Dermoscopy may be useful to differentiate erosive adenomatosis of the nipple from clinically similar diseases as mammary Paget's disease. Takashima et al. revealed dermoscopic features present in erosive adenomatosis of the nipple as linear cherry-red structures that might represent luminal openings amidst a light-reddish area, with collar-like orange veils at the periphery of the lesion. Instead, mammary Paget's disease usually shows light brown diffuse pigmentation, irregular black dots, peppering and irregular linear vessels, which are not present in erosive adenomatosis of the nipple.[2],[3]
Histopathologic examination can present various histologic features but usually shows ductal proliferation of gland-like structures within the stroma with well-circumscribed borders and no encapsulation.[1]
Mammography and/or breast ultrasound should always be done to rule out breast neoplasms; however, it is not useful to diagnose erosive adenomatosis of the nipple because of the similarity in the tissue density of the nipple, the surrounding skin and the underlying breast tissue.[1],[4]
The differential diagnosis is broad and includes mammary Paget's disease, squamous cell carcinoma of the nipple, eczema, psoriasis or skin infections.[1]
Treatment is often curative when a complete surgical excision is possible, minimizing local recurrence and is indicated as the first-line therapy. Unfortunately, it usually results in nipple amputation. Other alternatives include cryotherapy or Moh's micrographic surgery, especially indicated in young females to allow breastfeeding.[1],[5] Surgical excision was performed in our patient with no recurrences at a follow-up after 6 months.
Regular clinical breast follow-up after treatment is crucial, and includes annual screening mammography and/or breast ultrasonography. Incidental breast cancer (upto 17.6%) had been detected at the time of excision or at the site of biopsy. Nevertheless, it is still unknown if erosive adenomatosis of the nipple is a risk factor for the development of breast cancer. The incidence of erosive adenomatosis of the nipple in patients with breast cancer versus patients without breast cancer has not been studied, but the transformation of an erosive adenomatosis of the nipple into a breast cancer later cannot be completely excluded. Hence it is reasonable to encourage patients to maintain regular follow-up.[1]
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patient has given the consent for the images and other clinical information to be reported in the journal. The patient understand that name and initials will not be published and due efforts will be made to conceal identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
| 1. |
Spohn G, Trotter S, Tozbikian G, Povoski S. Nipple adenoma in a female patient presenting with persistent erythema of the right nipple skin: Case report, review of the literature, clinical implications and relevancy to health care providers who evaluate and treat patients with dermatologic conditions of the breast skin. BMC Dermatol 2016;16:4.
[Google Scholar]
|
| 2. |
Takashima S, Fujita Y, Miyauchi T, Nomura T, Nishie W, Hamaoka H, et al. Dermoscopic observation in adenoma of the nipple. J Dermatol 2015;42:341-2.
[Google Scholar]
|
| 3. |
Crignis GS, Abreu Ld, Buçard AM, Barcaui CB. Polarized dermoscopy of mammary Paget disease. An Bras Dermatol 2013;88:290-2.
[Google Scholar]
|
| 4. |
Wang C, Wang X, Ma R. Diagnosis and surgical treatment of nipple adenoma. ANZ J Surg 2015;85:444-7.
[Google Scholar]
|
| 5. |
Pasquali P, Freites-Martinez A, Fortuño A. Nipple adenoma: New images and cryosurgery treatment. Breast J 2016;22:584-5.
[Google Scholar]
|
Fulltext Views
5,799
PDF downloads
2,926





![[Figure - 1]](#fig_ijdvl_2019_85_3_307_237375_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2019_85_3_307_237375_f2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2019_85_3_307_237375_f3.jpg){kind=link}