Translate this page into:
Examination of circumscribed palmar hypokeratosis with line-field confocal optical coherence tomography: Dermoscopic, ultrasonographic and histopathologic correlates
2 Department of Medical, Dermatology Unit, Surgical and Neuro-Sciences, University of Siena, Siena, Italy
3 Department of Dermatology, Erasme Hospital, University of Brussels, Brussels, Belgium
4 Department of Dermatology, University Hospital of Saint-Etienne, Saint-Etienne, France
Correspondence Address:
Linda Tognetti
Department of Medical, Dermatology Unit, Surgical and Neuro-Sciences, University of Siena, Viale Bracci, Siena 53100
Italy
| How to cite this article: Tognetti L, Fiorani D, Suppa M, Cinotti E, Fontaine M, Marmol VD, Rubegni P, Perrot JL. Examination of circumscribed palmar hypokeratosis with line-field confocal optical coherence tomography: Dermoscopic, ultrasonographic and histopathologic correlates. Indian J Dermatol Venereol Leprol 2020;86:206-208 |
Sir,
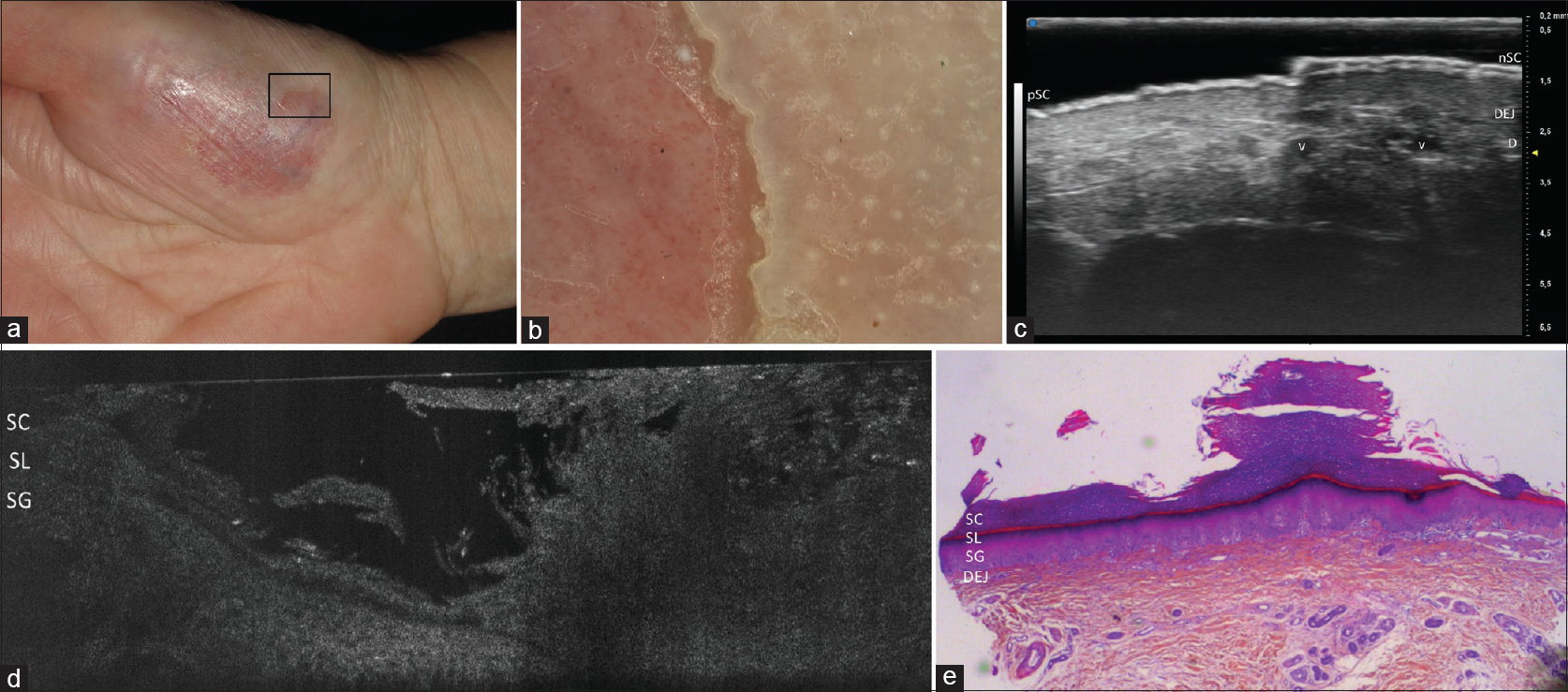
Three women presented with a solitary eroded patch on the thenar eminence of the right hand. One of the patients, aged 37 years, developed the asymptomatic erythematous rounded lesion of 1.5 × 2 cm with clear-cut raised borders about 2 years back [Figure - 1]a. Polarized dermoscopy (Lumenis, Visiomed) highlighted tiny and poorly visible dotted vessels and a vertical cut of the stratum corneum with a moth-eaten border [Figure - 1]b. Examination with a new line field optical coherence tomography (LC-OCT)[1] to a depth of ∼500 μm at the star-like edge revealed a 2/3 reduction in thickness of the stratum corneum [Figure - 1]c confirmed by histopathological examination [Figure - 1]d.
 |
| Figure 1: Patient 1: Clinical photograph (a), Polarized dermoscopy ×200 (b), line-field optical coherence tomography (LC-OCT) (c) and histopathologic examination (H and E, ×250) (d). Dermoscopy highlights dotted vessels over an erythematous background, along with and a vertical interruption and a motheaten profile (b). LC-OCT took at the stair-like edge revealed a 2/3 reduction in thickness of the stratum corneum (SC) that appeared as a homogenously and moderately reflective layer, unaltered stratum lucidum (SL) and stratum granulosum (SG) separated by a thin hypo-reflective dark linear space (c). These findings corresponded to the histopathological examination, which confirmed the diagnosis of circumscribed palmar hypokeratosis (d). |
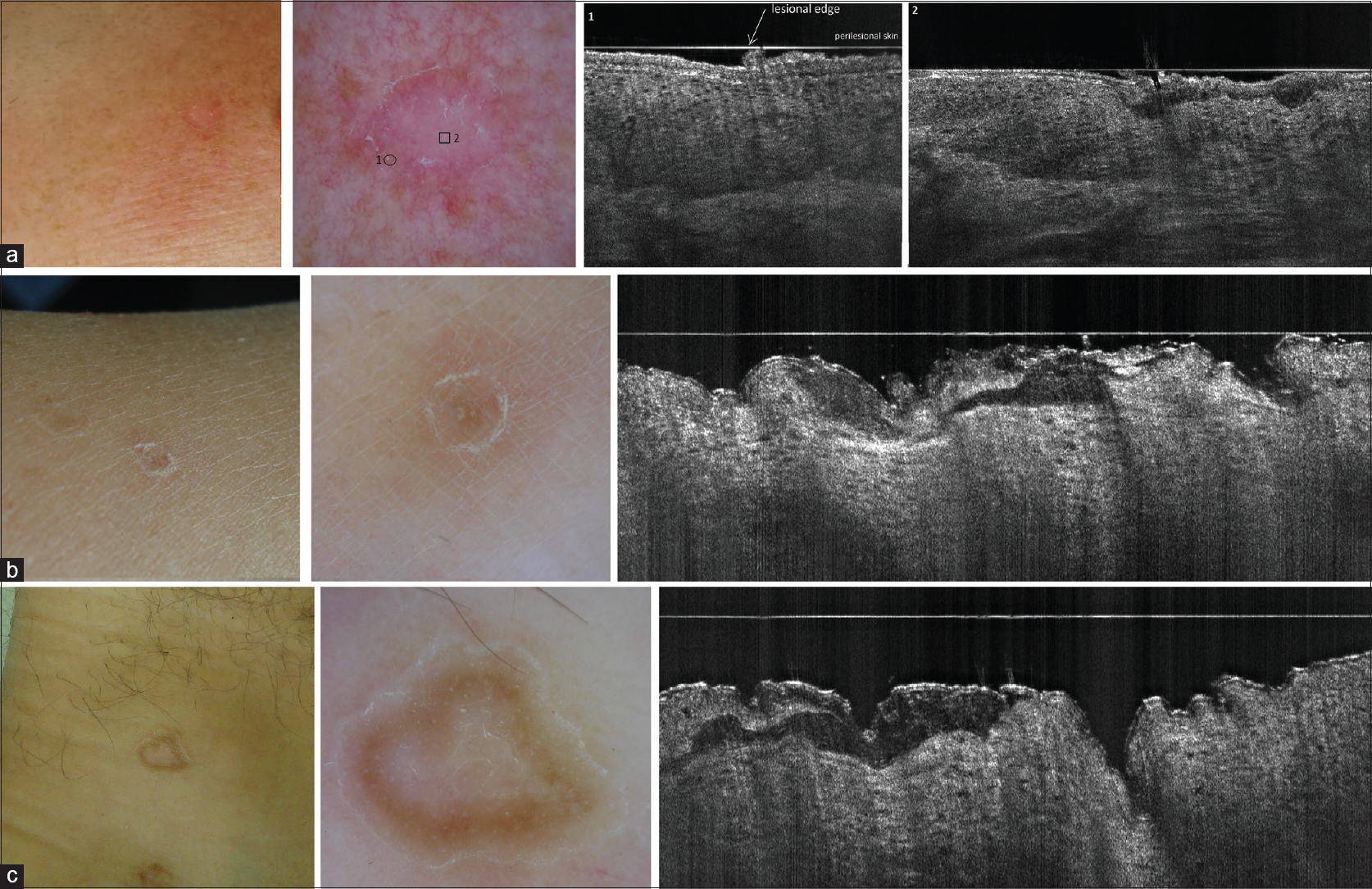
Patient 2, aged 57 years, showed an irregularly shaped erythematous lesion of 4.5 × 5 cm with clear-cut and focally scaling edges [Figure - 2]a. She referred cyclic inflammatory episodes with moderate burning sensation in the last 7 years. Polarized dermoscopy 30×, high-frequency ultrasound (HFUS) VEVO MD®, and LC-OCT were performed, followed by the biopsy of the lesion across its edge for histopathological correlation [Figure - 2]b, [Figure - 2]c. LC-OCT revealed in vivo that over the lesion, the SC was almost totally absent, while the stratum lucidum and stratum granulosum were intact [Figure - 2]d, corresponding to histopathology [Figure - 2]e. The same examinations were performed in patient 3, aged 67 years, showing the same dermoscopic and LC-OCT findings of a 2/3 reduction of the SC at lesional edge [Figure - 3].
 |
| Figure 2: Patient 2: Clinical photograph (a), polarized dermoscopy ×30 (b), high-frequency ultrasound (HFUS) (c), line-field optical coherence tomography (LC-OCT) (d) and histopathology (H and E, ×25) (e). HFUS revealed an intensely hyper-echogenic normal SC (nSC) with the classic double railway appearance pertaining to the perilesional skin as well as a hyper-echogenic band of pathological SC (pSC) overlying the lesion; moreover, dilated vessels (V) were visible in the papillary dermis (PD) (c). LC-OCT revealed intact stratum lucidum (SL) and sratum granulosum (SG), while the stratum corneum (SC) was almost totally absent; these findings were observed in the histological section (e). |
 |
| Figure 3: Patient 3: Clinical photograph (a), polarized dermoscopy×30 (b) and LC-OCT (c) taken at lesional border, showing a 2/3 reduction of the stratum corneum (SC). |
Circumscribed palmar hypokeratosis is a rare benign epidermal malformation, usually appearing on palms and soles, with about 50 cases described. The exact physiopathology is still unknown: the late onset of disease and the peculiar body site suggest a causative role for the repetitive local micro-traumatism in predisposed subjects.[2] Clinically, the differential diagnosis is essentially with a solitary roundish patch of Bowen disease and porokeratosis of Mibelli of the hand. However, Bowen disease is usually localized on the dorsum of the hand/fingers, has a dry erythemato-squamous surface with no raised white border and show peculiar dermoscopic features (i.e., glomerular vessels, dry scales, surface, small brown globules or structureless gray to brown pigmentation).[3] porokeratosis of Mibelli [Figure - 4] typically appears at pre-tibial surface or dorsal surface of the hands as a roundish patch with skin-colored/whitish center surrounded by a double “white track” scaling collarette with a brownish pigmentation in the inner side.[3] LC-OCT examination of he raised edge can help differentiating CPH form porokeratosis of Mibelli of the head [Figure - 4]a, leg [Figure - 4]b and ankle [Figure - 4]c.
 |
| Figure 4: Porokeratosis of Mibelli of the forehead (a), lower leg (b) and ankle (c): clinical photographs, polarized dermoscopy ×20 and line-field optical coherence tomography (LC-OCT). Under dermoscopy, the central atrophic epidermis shows white pink-whitish areas or red dots corresponding to enlarged capillary vessels. LC-OCT reveals the structure of the raised edge, where a thin column of tightly packed parakeratotic cells within a keratin-filled epidermal invagination (i.e, cornoid lamella), overlying an area of dyskeratotic and vacuolated cells. |
In addition, histopathological examination of CPH can be affected by artefacts occurred during slide preparation and/or staining. To avoid biopsy, noninvasive imaging tool including dermoscopy,[2] ultrasound[4] and OCT[5] were employed. The different dermoscopic features here observed are likely due to the different degree of thinning of the stratum corneum and of trauma-induced inflammation. HFUS was able to detect the stair-like interruption of the stratum corneum in both patients, showing an abrupt change of double to single entrance echo in the transition part, with a higher definition compared with cases examined with 20-MHz US.[4] Compared with standard OCT imaging,[5] LC-OCT imaging was able to reveal different level of stratum corneum reduction, with a stair-like vertical cut.[1] On the contrary, the oblique exfoliation of the stratum corneum usually seen in histologic section is likely to be due to stretching during slide preparation and fixation. Moreover, LC-OCT examination of porokeratosis of Mibelli cases highlighted a lower scaling edge than in CPH and a thinned atrophic epidermis and evident collagen bundles in the center of the lesion. Thus, LC-OCT could be proposed as an easy and rapid noninvasive technique to obtain real-time images, closely resembling a virtual biopsy section.[1]
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patients have given their consent for their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
| 1. |
Dubois A, Levecq O, Azimani H, Siret D, Barut A, Suppa M, et al. Line-field confocal optical coherence tomography for high-resolution noninvasive imaging of skin tumors. J Biomed Opt 2018; 23:1-9.
[Google Scholar]
|
| 2. |
Vilas Boas da Silva PT, Rodríguez-Lomba E, Avilés-Izquierdo JA, Ciudad-Blanco C, Suárez-Fernández R. Dermoscopic features of circumscribed palmar hypokeratosis. JAMA Dermatol 2017; 153:609-11.
[Google Scholar]
|
| 3. |
Lallas A, Errichetti E. Miscellaneous inflammatory diseases. In: Lallas A, Errichetti E, Ioannides D, editors. Dermoscopy in General Dermatology. 1st ed. Boca Raton: CRC Press; 2018.
[Google Scholar]
|
| 4. |
Polańska A, Bowszyc-Dmochowska M, Żaba R, Adamski Z, Pazdrowski J, Dańczak-Pazdrowska A, et al. High-frequency ultrasonography (20 MHz) in circumscribed palmar hypokeratosis – New observations. Arch Med Sci 2016; 12:1389-91.
[Google Scholar]
|
| 5. |
Abignano G, Kapadia A, Lettieri G, Goodfield M, Emery P, McGonagle D, et al. Use of optical coherence tomography for the diagnosis of preclinical lesions of circumscribed palmar hypokeratosis. Clin Exp Dermatol 2017; 42:192-5.
[Google Scholar]
|
Fulltext Views
3,482
PDF downloads
2,282





![[Figure - 1]](#fig_ijdvl_2020_86_2_206_277753_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2020_86_2_206_277753_f2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2020_86_2_206_277753_f3.jpg){kind=link}
![[Figure - 4]](#fig_ijdvl_2020_86_2_206_277753_f4.jpg){kind=link}