Translate this page into:
Extensive blue nevus of the pharynx
2 Department of Otolaryngology-Head and Neck Surgery, Tri Service General Hospital, National Defense Medical Center, Taipei, Taiwan, Republic of China,
Correspondence Address:
Yueng-Hsiang Chu
Department of Otolaryngology-Head and Neck Surgery, Tri Service General Hospital, National Defense Medical Center, 325, Sec. 2, Cheng-Kung Rd., Taipei 114, Taiwan, Republic of China
| How to cite this article: Lai WS, Hsu CH, Lee JC, Chu YH. Extensive blue nevus of the pharynx. Indian J Dermatol Venereol Leprol 2012;78:376-377 |
Sir,
The blue nevus is a benign, acquired melanocytic lesion that typically presents as an asymptomatic, slate-blue or blue-black, smooth-surfaced macule or papule, measuring less than 6 mm in diameter usually. [1] This lesion occurs mostly on the skin and rarely in the oral mucosa. [2] It is the most common type of nevus occurring in the oral cavity after intramucosal nevi and accounts for 19% to 36% of oral nevi. [3] Intraoral blue nevus was first described in 1959. Intraoral blue nevi occur most frequently on the hard palate, with the buccal mucosa being the second most common site. [2] We describe a case of blue nevus of the pharyngeal mucosa. To the best of our knowledge, this is the first report on blue nevi occurring in this unusual site.
A widespread blue-black plaque was detected in the oropharyngeal mucosa of a 58-year-old woman during a routine health examination. The patient was aware of the asymptomatic lesion for more than 20 years. She did not have pigmented lesions on any other part of the body and there was no history of trauma, infection, or addiction to tobacco. There were no pigmented lesions on the mucosal surfaces of the eyes, genitalia, or digestive tract. The results of the remaining clinical examinations were not remarkable. Endoscopy using a 0-degree rigid nasopharyngoscope and a 70-degree rigid laryngoscope revealed an irregularly shaped pigmented lesion in the oropharynx extending superiorly to the nasopharynx and inferiorly to the hypopharynx [Figure - 1]. The overlying mucosa was smooth, with no swelling or bulge. A tissue specimen was obtained from the posterior oropharyngeal wall by a punch biopsy. Histopathological examination of the obtained specimen showed infiltration of non-nested dermal dark spindle melanocytes associated with fibrosis, which are consistent with blue nevus [Figure - 2].
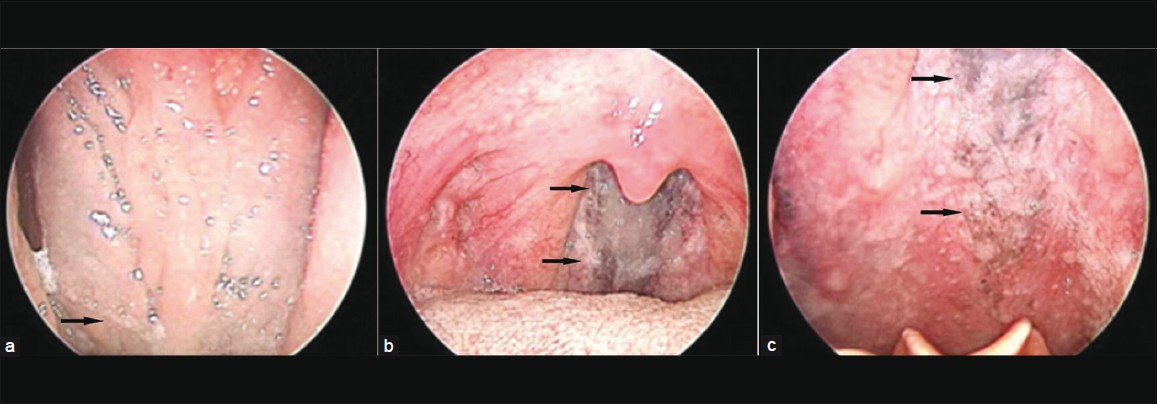 |
| Figure 1: The scope revealed an irregularly shaped pigmented area (black arrows) extending superiorly to the level of the nasopharynx (a) and inferiorly to the level of the hypopharynx (c), with the main part lying in the oropharynx (b) |
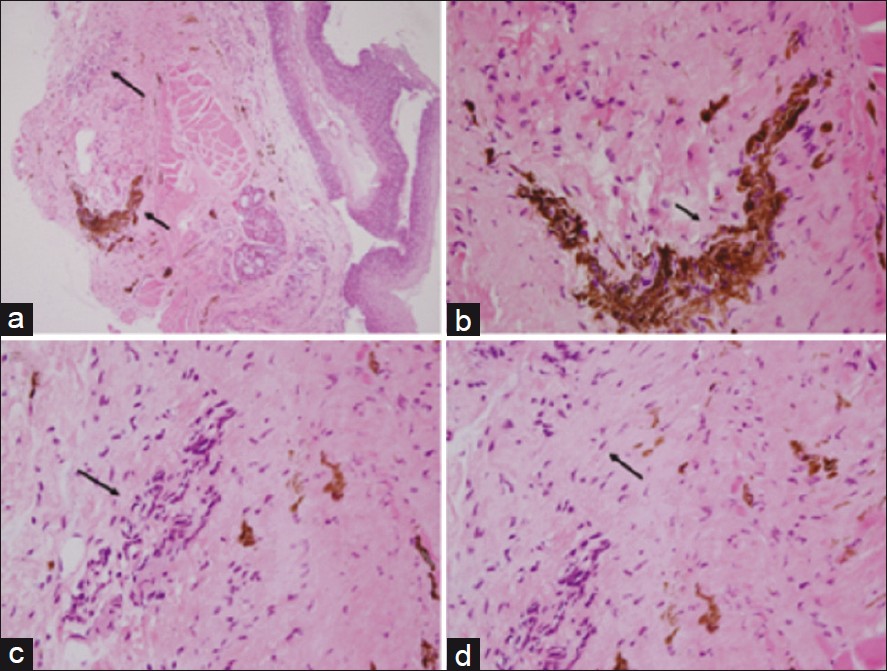 |
| Figure 2: H and E stained section of the lesion at ×40 magnification (a) and ×400 magnification (b, c and d). A benign proliferation of spindle melanocytes (a and c, long arrows), with prominent melanin pigmentation (a and b, short arrows). The spindle melanocytes were infiltrated with fibroblasts (d, arrow) |
Nevocytic nevi are protean lesions composed of several cell types arranged in a variety of histologic patterns. Dermal melanocytosis encompasses a spectrum of lesions including the following: (1) Mongolian spot, (2) nevus of Ota, (3) acquired nevus-of-Ota-like macules, (4) acquired dermal melanocytosis of the face and extremities, (5) nevus of Ito, (6) dermal melanocyte hamartoma, and (7) blue nevus. [4] The blue nevus is distinguished from the others on the basis of its histological presentation of a distorted dermis characterized by a greater concentration of dendritic melanocytes together with an increased fibrous tissue and melanophage. However, the lesions listed above are histologically similar to some extent. Thus, the diagnosis of dermal melanocytosis should be confirmed by taking into consideration both the histological picture and the clinical features of the lesion such as size, surface, and location.
Intraoral melanocytic nevi are uncommon and mostly occur on the palate or gingiva, although any mucosal site may be involved. The most common melanocytic nevi occurring in the oral cavity are of the intramucosal type (63%), followed by blue nevi (19%), compound nevi (9%), junction nevi (5%), and combined nevi (4%). [5]
Blue nevi generally occur on the skin of the hands, feet, and buttocks; however, in rare instances, they may occur in mucous membranes, including the oral mucosa. In most cases, blue nevi occurring in the oral mucosa are less than 10 mm in diameter and located on the hard palate. The common blue nevus, which is the most frequent subtype seen in the oral cavity, is characterized by the intramucosal proliferation of elongated, bipolar, spindle-shaped melanocytes that are often grouped in short fascicles arranged parallel to the overlying epithelium. Histologically, the pigmented spindle melanocytes can also be found in malignant melanoma and Spitz nevus.
In the differential diagnosis of the lesion, a melanoma arising form the pharyngeal mucosa is first considered, the other diseases include pseudomelanoma (recurrent melanocytic nevus), nicotine keratoses, drug induced pigmentation, oral melanoacanthoma, pigmentation induced by dental amalgams, nevus of o0 ta, and Mongolian spots, etc. The monomorphic and bland appearance of the proliferating cells and the absence of both mitotic activity and an infiltrating growth pattern ruled out melanocytic malignancy. In addition, the bluish pigmentation lesion in the pharyngeal mucosa should be distinguished from different types of hemangiomas, such as blue rubber-bleb nevus. In this case, the patient showed neither bluish vascular nevi of the skin nor hemangiomas of the gastrointestinal tract.
In conclusion, for both cutaneous and noncutaneous blue nevi, the preferred treatment is surgical excision, which generally results in a cure. However, a complete excision was not possible in this case because of the extent and location of the lesion. Melanotic lesions are rare in the pharyngeal mucosa. Diagnostic ENT endoscopes and ultrasonogrpahy in this case were very illustrative in demonstrating the extensive blue cell nevus of the pharynx, which was never hitherto formerly delineated.
| 1. |
Scofield HH. The blue (Jadassohn-Tieche) nevus: A previously unreported intraoral lesion. J Oral Surg Anesth Hosp Dent Serv 1959;17:4-14.
[Google Scholar]
|
| 2. |
Fistarol SK, Itin PH. Plaque-type blue nevus of the oral cavity. Dermatology 2005;211:224-33.
[Google Scholar]
|
| 3. |
Buchner A, Hansen LS. Pigmented nevi of the oral mucosa: A clinicopathologic study of 36 new cases and review of 155 cases from the literature. Part II: Analysis of 191 cases. Oral Surg Oral Med Oral Pathol 1987;63:676-82.
[Google Scholar]
|
| 4. |
Scolyer RA, Thompson JF, Stretch JR, Sharma R, McCarthy SW. Pathology of melanocytic lesions: New, controversial, and clinically important issues. J Surg Oncol 2004;86:200-11.
[Google Scholar]
|
| 5. |
Buchner A, Hansen LS. Pigmented nevi of the oral mucosa: A clinicopathologic study of 32 new cases and review of 75 cases from the literature. Part I. A clinicopathologic study of 32 new cases. Oral Surg Oral Med Oral Pathol 1979;48:131-42.
[Google Scholar]
|
Fulltext Views
2,982
PDF downloads
1,806





![[Figure - 1]](#fig_ijdvl_2012_78_3_376_95467_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2012_78_3_376_95467_f2.jpg){kind=link}