Translate this page into:
Facial unilateral angiofibromas: A postzygotic tuberous sclerosis like mutation
Correspondence Address:
Adone Baroni
c/o II Policlinico, Edificio 3, Quarto piano, Via Pansini 5 - 80131 Napoli
Italy
| How to cite this article: Baroni A, Piccolo V, Montesarchio G, Faccenda F, Russo T, Satriano RA. Facial unilateral angiofibromas: A postzygotic tuberous sclerosis like mutation. Indian J Dermatol Venereol Leprol 2011;77:731 |
Sir,
Facial angiofibromas are flesh colored or red papules located centrofacially, especially on the nose, cheeks, and chin and represent a major criterion of tuberous sclerosis (TS). Unilateral facial angiofibromas (UFA) have been occasionally reported in literature. We present a case of UFA in a 36-year-old patient without other features of TS, review each case of previously described UFA and discuss the possible pathogenetic mechanism supporting the occurrence of these skin tumors.
A 36-year-old man was referred to our department for evaluation of multiple reddish-orange papules affecting the left side of nose, cheek, and chin [Figure - 1], appeared 30 years earlier and increasing in number during puberty. There were no shagreen patches (SP), periungual fibromas (PF), hypopigmented macules (HM), or forehead plaques (FP). A biopsy specimen obtained from a lesion of the cheek showed dermal fibrosis, a mild hyperkeratosis and, in the subepidermal dermis, a proliferation of angiectatic vessels, some of which had a thin wall [Figure - 2]. Histopatological examination related to clinical features was compatible with the diagnosis of facial angiofibromas (FA), enabling us to rule out fibrofolliculomas and trichoepitheliomas. The patient was born from nonconsanguineous parents after a normal pregnancy and delivery. He had a normal psychomotor development and there was no history of convulsions, mental retardation, pulmonary lesions, renal lesions, retinal abnormalities, or cardiac arrhythmias. There was no family history of similar cutaneous lesions or seizures. Further investigations were performed to exclude other potential manifestations of tuberous sclerosis (TS). Cortical tubers (CT) and subependymal nodules (SN) were excluded by magnetic resonance imaging (MRI). Abdomen ultrasonography and ophthalmological examination were unremarkable. Genetic study was not available. After 1 year of follow-up, no further skin lesions appeared. Some cases of facial angiofibromas have been related to multiple endocrine neoplasia 1 (MEN 1) and neuorofibromatosis, but none of them were reported as unilateral. Moreover, MEN 1 was ruled out because of the negativity of laboratory endocrinological screenings (parathyroid, pancreatic, and pitutitary hormones). TS is an autosomal dominant neurocutaneous disorder, related to the mutation of TSC1 and TSC2 located on 9q34 and 16p13, respectively. These genes normally express a tumor-suppressing function, but, once mutated, they stop carrying out their function and the tumors of TS occur. [1],[2],[3],[4],[5] Skin lesions of TS include FA, UF, SP, FP, HM, and confetti spots. FA represent the most frequent cutaneous sign of TS, [1],[2],[3],[4],[5] symmetrically distributing on the nose, chin and cheeks, sometimes involving forehead and eyelids. [1] Unilateral distribution of FA has been previously reported in a few cases. [1],[2],[3],[4],[5] To date, the clinical significance of unilateral FA (UFA) is unknown, but several hypotheses trying to explain this phenomenon have been advanced. Graham suggested the fibrous papules of the nose to be constituted by a special form of regressive nevus cells, mentioning increased melanocytes in the dermoepidermal junction in some of the lesions. [1] Other authors supposed that UFA may be the first manifestation of TS, supported by the report of patients with UFA, which developed extra-cutaneous manifestations of TS. [1],[2],[3],[4],[5] UFA are actually considered as a segmental, genetically defined form of TS. [1],[2],[3],[4],[5] Occurrence of UFA has been postulated to be analogous to segmental neurofibromatosis type V in which the expression of disease is restricted to a unilateral segment of the body, whose genetic mechanism of is a postzygotic mutation leading to an abnormal phenotypic expression only in the affected segment. In conclusion, UFA may represent a segmental form of TS probably as a consequence of cutaneous mosaicism in which a postzygotic mutation has occurred. However, in our opinion further investigations at time of diagnosis and a periodic follow-up for patients with UFA without other manifestations of TS are necessary for the possibility they have to develop additional signs of the disease.
 |
| Figure 1: Physical examination revealed about 25−30 reddish-orange papules, 1 to 3 mm in diameter affecting the left side of nose, cheek, and chin |
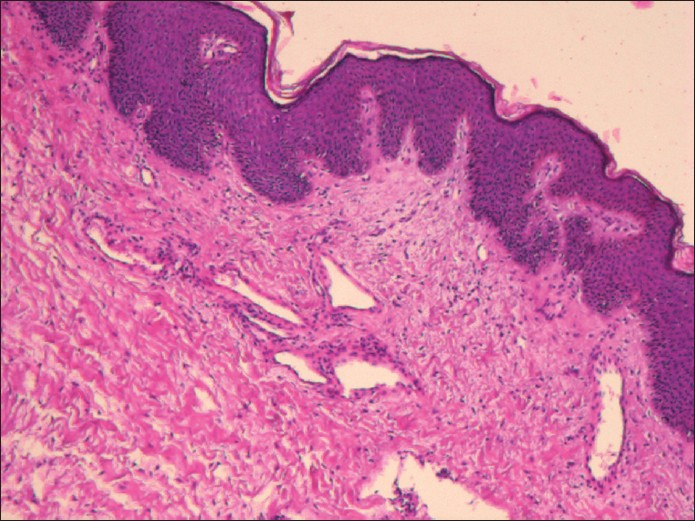 |
| Figure 2: Histopathology showed dermal fibrosis, a mild hyperkeratosis, and in the subepidermal dermis, a proliferation of angiectatic vessels. (H and E, ×20) |
| 1. |
Camprubi M, Balaguer A, Azon Masoliver A, Jiménez Feijoo R, Escribano Subias J. Unilateral facial angiofibromas; A review of the literature. Pediatr Dermatol 2006;23:303-5.
[Google Scholar]
|
| 2. |
Trauner MA, Ruben BS, Lynch PJ. Segmental tuberous sclerosis presenting as unilateral facial angiofibromas. J Am Acad Dermatol 2003;49:S164-6.
[Google Scholar]
|
| 3. |
Alonso Pacheco ML, Zambrano Centino B, de Eusebio Murillo E, Jaén Olasolo P, Cuevas Santos J. Angiofibromas faciales múltiples unilaterales. Med Cutan Iber Lat Am 2004;32:249-3.
[Google Scholar]
|
| 4. |
Silvestre JF, Banuls J, Ramón R, Guijarro J, Botella R, Betlloch I. Unilateral multiple facial angiofibromas: A mosaic form of tuberous sclerosis. J Am Acad Dermatol 2000;43:127-9.
[Google Scholar]
|
| 5. |
Hall MR, Kovach BT, Miller JL. Unilateral facial angiofibromas without other evidence of tuberous sclerosis: Case report and review of the literature. Cutis 2007;80:284-8.
[Google Scholar]
|
Fulltext Views
2,991
PDF downloads
2,317





![[Figure - 1]](#fig_ijdvl_2011_77_6_731_86510_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2011_77_6_731_86510_f2.jpg){kind=link}