Translate this page into:
Giant porokeratosis
Correspondence Address:
Dincy Peter Christudas Valsamma
Department of Dermatology, Venereology and Leprosy, Christian Medical College and Hospital, Vellore - 632 004
India
| How to cite this article: Raychaudhury T, Valsamma DP. Giant porokeratosis. Indian J Dermatol Venereol Leprol 2011;77:601-602 |
A 45-year-old gentleman from West Bengal, India, presented with hyperkeratotic irregular plaques of variable sizes over the face, arms, chest wall and back. He was a carpenter, with no history to suggest excessive sun exposure. These lesions were present for the past 15 years, and were progressively increasing in size. The largest lesion was present over the back, with thick focal hyperkeratotic areas that used to shed thick hard scales on acquiring larger sizes. His father had similar lesions while his son had started developing these lesions since 10 years of age [Figure - 1]. On dermatologic examination, he had a 13 x 12 cm irregular plaque over the mid-back, with central atrophy, variegate colors with few keratotic papules in the center of the plaque and a peripherally located hyperkeratotic wall [Figure - 2]. The hyperkeratotic wall over the inferior border measured from 1.2 to 1.7 cm in height. There were multiple smaller annular plaques with a less distinctive border noted over the face and arms. A three-site histopathology examination was performed to confirm the diagnosis of porokeratosis and rule out associated squamous cell carcinoma or Bowen′s disease, including tissue sampling from the differently colored areas in the center of the plaque. The biopsy findings of marked hyperkeratosis, cornoid lamella without any evidence of malignancy [Figure - 3] along with clinical features suggested a diagnosis of giant porokeratosis co-existing with disseminated superficial porokeratosis.
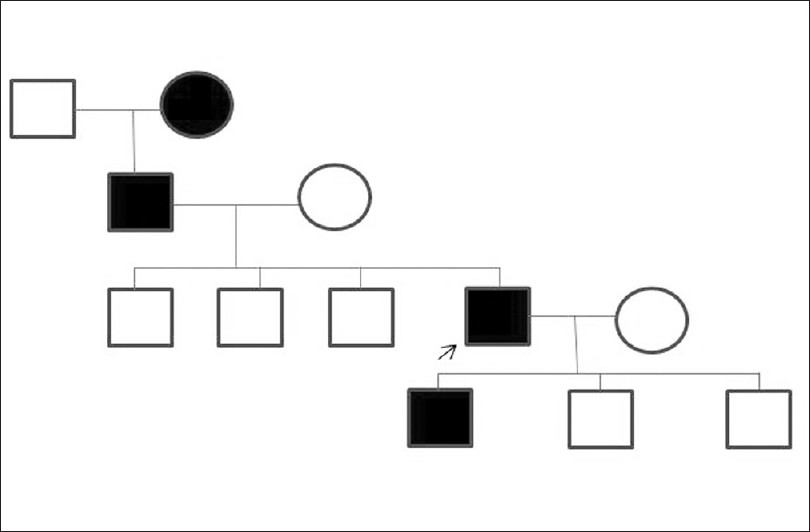 |
| Figure 1: Pedigree chart of patient |
 |
| Figure 2: Giant porokeratosis noted over the back |
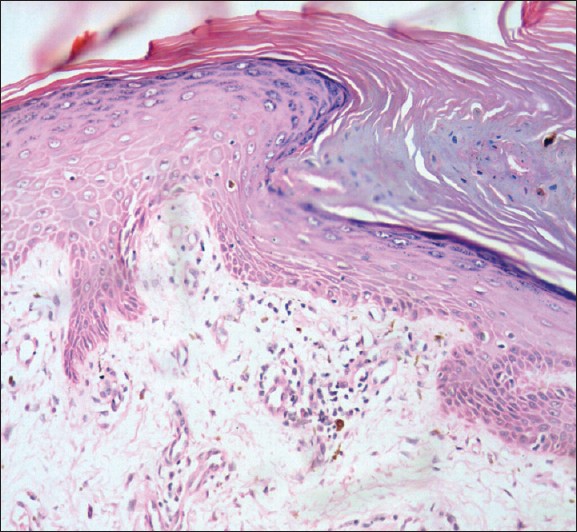 |
| Figure 3: Histopathology of the superior margin of lesion showing invagination of the epidermis and cornoid lamella, consistent with porokeratosis (H and E, ×200) |
Porokeratosis is a rare, genetically determined autosomal dominant disorder of epidermal keratinization characterized by lesions with keratotic borders corresponding histopathologically to compact columns of parakeratotic cells called cornoid lamellae that extend through the stratum corneum. The clinical variants include porokeratosis of Mibelli, giant porokeratosis, disseminated superficial actinic porokeratosis, disseminated superficial porokeratosis, linear porokeratosis, palmoplantar porokeratosis, and punctate porokeratosis. In 1893, the classic lesions of porokeratosis were first described by Mibelli as single or multiple annular and gyrate plaques with central atrophy and elevated keratotic borders containing a longitudinal furrow.
Giant porokeratosis is considered to be a morphological variant of porokeratosis of Mibelli by some authors, while others consider it as a distinct entity. The lesions may vary from 10 to 20 cm in diameter, and the hyperkeratotic walls raised greater than 1 cm. Variants may co-exist in the same individual occasionally. The pathogenesis of porokeratosis is proposed to be a mutant clone of peripherally expanding epidermal cells, leading to formation of cornoid lamella at the boundary between the clonal population and normal keratinocytes. Squamous cell carcinoma and Bowen′s disease have been reported in giant porokeratosis, including in Indian patients.
Fulltext Views
3,668
PDF downloads
2,131





![[Figure - 1]](#fig_ijdvl_2011_77_5_601_84072_u1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2011_77_5_601_84072_u2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2011_77_5_601_84072_u3.jpg){kind=link}