Translate this page into:
Giant porokeratosis of Mibelli with squamous cell carcinoma
2 Skin Research Center, Shahid Beheshti University of Medical Sciences, Shohada-e Tajrish Hospital, Tehran, Iran
Correspondence Address:
Maryam Ranjbar
Skin Research Center, Shahid Beheshti University of Medical Sciences, Shohada-e Tajrish Hospital, Tehran
Iran
| How to cite this article: Ehsani AH, Shakoei S, Ranjbar M. Giant porokeratosis of Mibelli with squamous cell carcinoma. Indian J Dermatol Venereol Leprol 2014;80:96 |
Sir,
Porokeratosis of Mibelli is an uncommon keratinization disorder. [1] Malignant transformation into squamous, bowenoid or basal cell carcinoma has been described in all forms of porokeratosis with the highest risk for the linear form. [2]
We describe a patient with an extraordinary large-sized porokeratosis of Mibelli, complicated with a lesion of squamous cell carcinoma.
A 57-year-old woman presented with an erythematous pruritic irregular plaque on her right lower extremity since she was 7-year-old. She had a history of burns when she was in her 6 th year. The plaque developed approximately 1 year after the remission of the burn with the initial size of 2 cm × 2 cm with no change until 18 years later; but at the time of her first pregnancy and childbirth, it started to extend gradually to a final size of 25 cm × 50 cm when she was 25 years old. She experienced stinging, pain and itching at the site of the lesion.
After confirming the diagnosis of porokeratosis of Mibelli based on her last biopsy in 2001, she used topical steroids for 1 year irregularly, which was discontinued because no changes were observed in her signs or symptoms. She had been using only topical moisturizer and oral antihistamines for several years since then.
The lesion was stable with no more change subsequently until the time when she referred to our center with a well-circumscribed ulcerative nodule on her leg, which arised 7 months before presenting to us.
Physical examination revealed a 50 cm × 25 cm scaly erythematous plaque on the anterior, posterior and lateral side of the lower extremity extending from her leg to her thigh with an approximately raised keratotic border along with atrophy and hair loss at the center of the lesion. A well-defined erythematous nodule with a size of 4 cm × 4 cm was accompanied by hemorrhagic crusts and some purulent discharge on the surface of the lesion [Figure - 1]. Her general physical examination was quite normal and also, there was no palpable inguinal lymph node on her physical examination.
 |
| Figure 1: The scaly erythematous plaque with raised keratotic border along with atrophy and hair loss at the center of the lesion. A well-defined erythematous nodule with a size of 4 cm × 4 cm on the surface of the lesion |
There was no involvement of any other parts of her body. The family history of similar lesions was negative. Her medical history revealed no specific drug other than some supplements. She had a positive history of cigarette smoking for 15 years (2/day). Routine blood tests and chest X-ray were completely normal.
The histopathological examination of lesions showed a keratin-filled epidermal invagination with a parakeratotic column: The so-called cornoid lamella; it also showed loss of the granular layer, within the parakeratotic column. These histological findings suggested the diagnosis of porokeratosis of Mibelli and the biopsy of nodules showed a moderately differentiated squamous cell carcinoma consisting of hyperchromatic nuclei, some atypical mitotic figures, keratinization of individual cells and horn pearls [Figure - 2] and [Figure - 3]. After confirming the diagnosis, patient was referred to a surgeon and the lesion was excised with free margins.
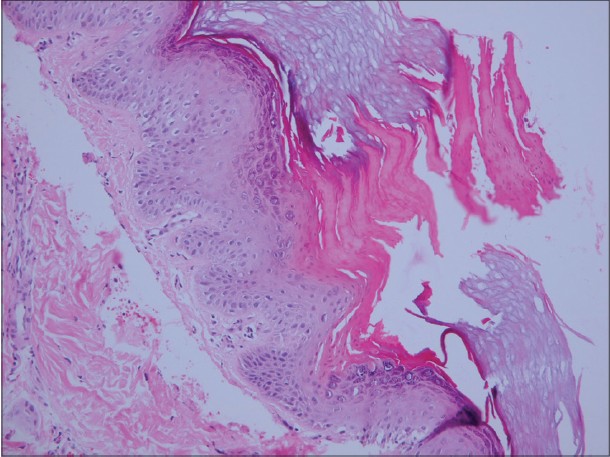 |
| Figure 2: A keratin-filled epidermal invagination with rises a parakeratotic column the so-called cornoid lamella; it also showed loss of the granular layer, within the parakeratotic column (H and E, × 40) |
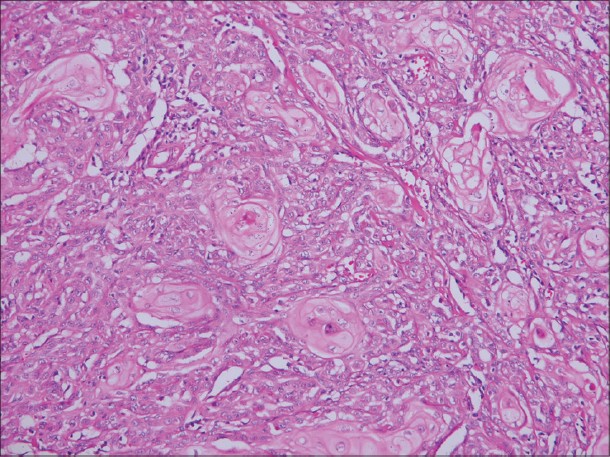 |
| Figure 3: The histopathological examination of the nodule showed hyper chromatin of the nuclei, some atypical mitotic figures, keratinization of individual cells and horn pearls consistent with a moderately differentiated squamous cell carcinoma (H and E, × 400) |
Porokeratosis is clinically characterized by asymptomatic or mild pruritic keratotic papules surrounded by a raised keratotic border. The pathogenesis of porokeratosis of Mibelli is not well-established yet. Various risk factors involved in the development of porokeratosis include genetic inheritance, [1] immunosuppression, [1],[3] ultraviolet radiation and sun exposure, [1] particularly immunosuppression. [4]
This disorder usually appears in childhood although adult onset has also been reported, especially following immune suppression with different etiologies. The lesions often have a predilection to the extremities, but can also develop on other sites such as neck, shoulders, face and genitalia. [1]
The factors demonstrated to be associated with a higher risk of malignant transformation include: Duration and size of the lesions, age of patient, large lesions on the extremities and linear type [4] as well as multiple patterns of porokeratosis. [2]
To the best of our knowledge, the risk for malignant transformation of porokeratosis of Mibelli has been reported to be 7.5-11%. [2]
In this case, our patient has some potential risk factors such as her age along with the long duration and large size, all of which strongly justify its conversion to squamous cell carcinoma. On the other hand, it is noteworthy to mention that the size of her lesion was stable until her first pregnancy while it started to enlarge immediately after her first childbirth, which may refer to the probable immune suppression [5] women generally experience during pregnancy.
To the best of our knowledge, several large lesions of porokeratosis of Mibelli have been reported to date as giant ones. [2] The largest lesion had a size of 18 cm × 13 cm, [6] whereas the presenting case introduces a huge lesion of porokeratosis with a size of 25 cm × 50 cm, which is extremely rare.
In general, we can conclude that patients with long-standing and large lesions of porokeratosis should be monitored regularly to detect malignant changes.
| 1. |
Odeyinde S, Belcher H. Isolated single digit porokeratosis of mibelli: An unusual case. Dermatol Online J 2012;18:13.
[Google Scholar]
|
| 2. |
Sengupta S, Das JK, Gangopadhyay A. Multicentric squamous cell carcinoma over lesions of porokeratosis palmaris et plantaris disseminata and giant porokeratosis. Indian J Dermatol Venereol Leprol 2005;71:414-6.
[Google Scholar]
|
| 3. |
Pérez-Crespo M, Betlloch I, Lucas-Costa A, Bañuls-Roca J, Niveiro de Jaime M, Mataix J. Unusual evolution of giant porokeratosis developing in two renal transplant patients. Int J Dermatol 2008;47:759-60.
[Google Scholar]
|
| 4. |
Sasson M, Krain AD. Porokeratosis and cutaneous malignancy. A review. Dermatol Surg 1996;22:339-42.
[Google Scholar]
|
| 5. |
Mor G, Cardenas I. The immune system in pregnancy: A unique complexity. Am J Reprod Immunol 2010;63:425-33.
[Google Scholar]
|
| 6. |
Ma DL, Vano-Galvan S. Squamous cell carcinoma arising from giant porokeratosis. Dermatol Surg 2009;35:1999-2000.
[Google Scholar]
|
Fulltext Views
3,477
PDF downloads
2,892





![[Figure - 1]](#fig_ijdvl_2014_80_1_96_125519_u1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2014_80_1_96_125519_u2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2014_80_1_96_125519_u3.jpg){kind=link}