Translate this page into:
Hand, foot and mouth disease caused by Coxsackie viruses A6 and A16 in Assam, Northeast India: A need for surveillance
2 Pediatrics Department, Assam Medical College and Hospital, Dibrugarh, Assam, India
Correspondence Address:
Mandakini Das
Research Scientist I (NM), Regional Virus Research Diagnostic Laboratory, ICMR-Regional Medical Research Centre, N.E. Region, Post Box-105, Dibrugarh - 786 001, Assam
India
| How to cite this article: Borkakoty B, Das M, Jakharia A, Bhattacharya C, Bora C, Baruah PJ, Biswas D. Hand, foot and mouth disease caused by Coxsackie viruses A6 and A16 in Assam, Northeast India: A need for surveillance. Indian J Dermatol Venereol Leprol 2020;86:105 |
Sir,
Hand, foot and mouth disease is a common childhood viral infection characterized by fever and papulovesicular eruptions on hands, feet and mouth and also involves buttocks in many cases.[1] It is caused by members of the family Picornaviridae in the genus Enterovirus.[2]
The first report of hand, foot and mouth disease outbreak in India was in 2004 from Calicut.[3] After 3 years, the first large-scale outbreak occurred in 2007 from Kolkata and in the surrounding areas of the eastern state, West Bengal.[4] Since then, many small-scale outbreaks have been repeatedly reported from different places based on clinical description.[5] However, there are no laboratory-confirmed reports of hand, foot and mouth disease from Northeast India. This is the first report of laboratory-confirmed hand, foot and mouth disease outbreak from Assam, Northeast India. In 2014, the Pediatric Department of Assam Medical College and Hospital, Dibrugarh and nearby tertiary hospitals in Dibrugarh and Tezpur reported cases with hand, foot and mouth disease symptoms. Samples were collected from patients with hand, foot and mouth disease symptoms in 2014 for molecular characterization as and when possible.
A total of 10 throat samples were collected for laboratory confirmation from clinically diagnosed cases of hand, foot and mouth disease in 2014 from Outpatient Department, Tezpur University Hospital, Tezpur and Outpatient Department, Assam Medical College and Hospital, Dibrugarh. The cases ranged from 1 to 40 years and 6/10 (60%) cases were below the age of 10 years. The most common symptom was fever (8/10, 80%), followed by sore throat (6/10, 60%), itchy skin (8/10, 80%) and anorexia (3/10, 30%). Clinically, dermatologic presentation included papulovesicular lesions on hands and feet. Oral lesions were found in 7 (70%) cases. Sites of involvement were the inner side of the lips, gums, tongue and the hard palate. Usually, 1–3 small erythematous erosions of 4–5 mm size were noted. Two cases had diffuse inflammation over larger areas of gums and mouth ulcerations. An atypical site of involvement with lesions in knee was observed in one case. The patterns of the phenotype of hand, foot and mouth disease cases included in the study are shown in [Figure - 1] and [Figure - 2].
 |
| Figure 1: Oral ulcer in the soft palate and tip of the tongue |
 |
| Figure 2: Erythematous papular vesicles in hand and foot of child |
Out of the 10 cases, six were found to be enterovirus positive by reverse transcription polymerase chain reaction. Molecular typing and subsequent sequencing of the positive samples confirmed two cases as Coxsackie virus serotype A6 (CV-A6) and two as Coxsackie virus serotype A16 (CV-A16), and two were non-typeable Enterovirus (EntV) [Figure - 3]. The CV-A6 cases were reported from Tezpur district and CV-A16 cases were reported from Dibrugarh district. Further, phylogenetic analysis of the 5′ UTR region of CV strains in the current study (GenBank: KT275248 to KT275251) with the reference sequence from NCBI revealed that the consensus sequences of CV A6 from Tezpur, Assam, shared 98–99% nucleotide identity with China strain in 2012 (GenBank: KJ541169) and were also close to those circulating in Finland in 2008 (GenBank: KP144346). In the subsequent year, in 2015, sporadic cases of hand, foot and mouth disease were reported from schools in and around Dibrugarh, and the samples were collected. Two samples were found to be positive for CV-A16.
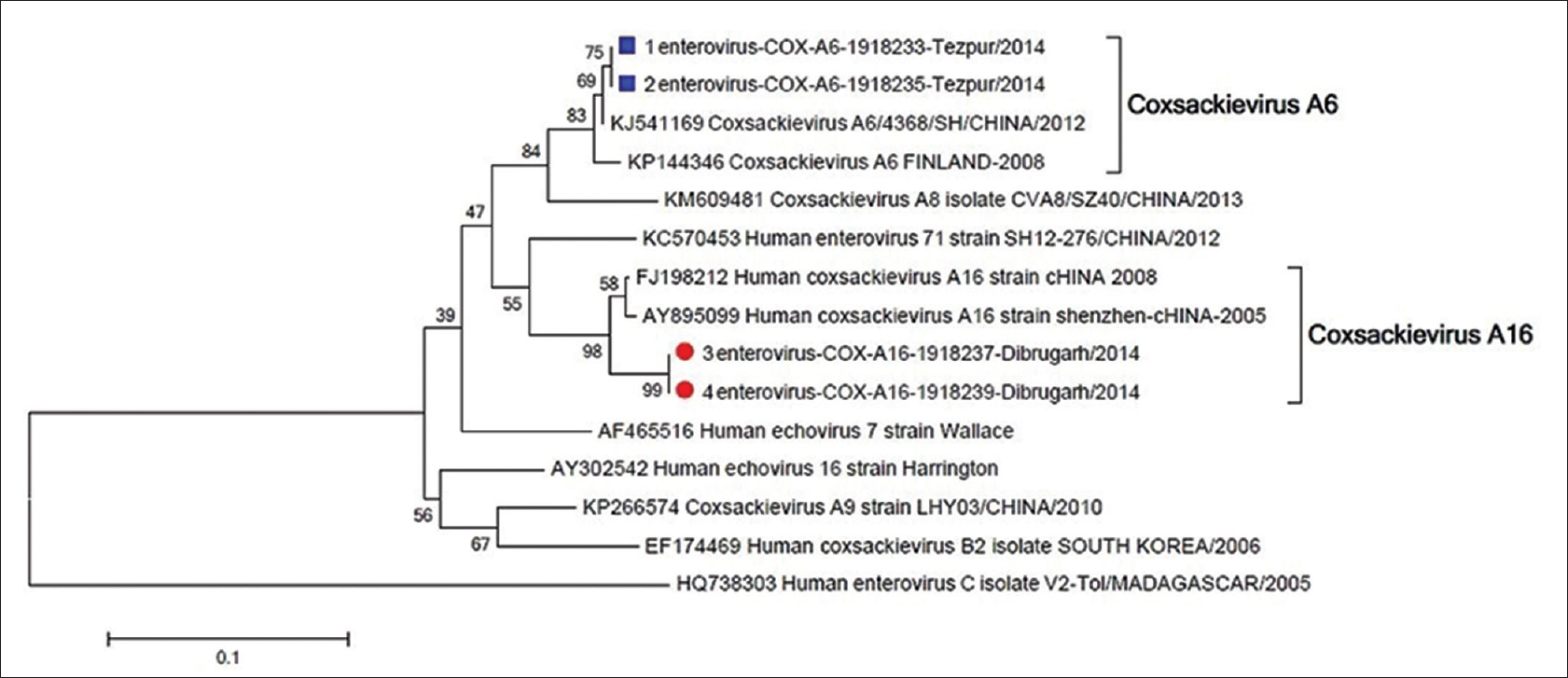 |
| Figure 3: Phylogenetic analysis of 5'-UTR region of Coxsackie virus using maximum likelihood method. The bootstrap consensus tree inferred from 1000 replicates is taken to represent the evolutionary history of the taxa analyzed. Hand, foot and mouth disease samples from Tezpur, Assam are represented in square boxes and hand, foot and mouth disease samples from Dibrugarh, Assam are represented in circles |
The disease course of CV-A6 is different from CV-A16 and EV-71. Hand, foot and mouth disease patients with CV-A6 infection have been reported to have more widespread skin lesions when compared with CV-A16 or EV-71 infection.[6] In our study too, CV-A6 patients reported more skin lesions beyond the typical sites for hand, foot and mouth disease, including trunk and perioral area.
Incidentally, on retrospective analysis of the medical records during September 2014 by our team, more than 1000 cases with hand, foot and mouth disease clinical symptoms were observed. Surveillance for hand, foot and mouth disease was done in 2015 and only sporadic cases were reported from tertiary hospitals in Dibrugarh and Tezpur with a quiescent phase in 2016. Although no cases of neurological or pulmonary manifestations were detected so far and all the cases improved spontaneously without any requirement for hospitalization, spread of the disease over larger parts of the country reminds the pre-epidemic periods of China and Taiwan. This necessitates the need for awareness as all previous cases of severe outbreaks worldwide followed many years of milder attacks, intermittent periods of quiescence and progressively larger areas of involvement. The reported hand, foot and mouth disease outbreak in Assam, Northeast India, which is in close geographical proximity to China and other Southeast Asian countries with previous incidence of fatal outbreaks sends an alert that the disease has now acquired the potentiality to affect larger parts of the country. The CV-A6 serotype identified in Tezpur district shares 98–99% nucleotide homology with CV-A6 strain of China which caused a large outbreak of hand, foot and mouth disease in 2012 and CV-A6 in Finland in 2008. Unfortunately, awareness among the primary level doctors or medical staff regarding the disease is limited. Health awareness among school teachers, school authorities, daycare centers about the contagious nature of hand, foot and mouth disease would help in limiting the disease outbreak. Moreover, because of the atypical presentation of CV-A6-associated hand, foot and mouth disease, clinical vigilance is needed to recognize emerging regional outbreaks. Further, identification of common hand, foot and mouth disease strains will help in vaccine development against these new viral agents such as CV-A6 and CV-A16 identified in the present study. There are certain limitations in our study as to the limited sample size used for molecular characterization. However, with the limited sample size, this study provides the first laboratory-confirmed report of hand, foot and mouth disease from Northeast India along with first-hand information on the circulating genotypes. Further studies with larger sample size can help to understand the disease pattern better. With this background, we report this outbreak of hand, foot and mouth disease, in the hope that it will help to embark upon an early survey on epidemiological trends of the diseases in India and Northeast India to predict the disease behavior so that control measures can be effectively planned to abort or halt a prospective severe outbreak.
Acknowledgement
This work was supported by the Regional Virus Research Diagnostic Laboratory, Dibrugarh, Assam, a scheme under Department of Health Research, Government of India.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patients have given their consent for their images and other clinical information to be reported in the journal. The patient understands that name and initials will not be published and due efforts will be made to conceal identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Department of Health Research, Govt.of India.
Conflicts of interest
There are no conflicts of interest.
| 1. |
Duff MF. Hand-foot-and-mouth syndrome in humans: Coxackie A10 infections in New Zealand. Br Med J 1968;2:661-4.
[Google Scholar]
|
| 2. |
Chen JF, Zhang RS, Ou XH, Chen FM, Sun BC. The role of Enterovirus 71 and coxsackievirus A strains in a large outbreak of hand, foot, and mouth disease in 2012 in Changsha, China. Int J Infect Dis 2014;28:17-25.
[Google Scholar]
|
| 3. |
Sasidharan CK, Sugathan P, Agarwal R, Khare S, Lal S, Jayaram Paniker CK. Hand-foot-and-mouth disease in Calicut. Indian J Pediatr 2005;72:17-21.
[Google Scholar]
|
| 4. |
Sarma N, Sarkar A, Mukherjee A, Ghosh A, Dhar S, Malakar R. Epidemic of hand, foot and mouth disease in West Bengal, India in August, 2007: A multicentric study. Indian J Dermatol 2009;54:26-30.
[Google Scholar]
|
| 5. |
Gopalkrishna V, Patil PR, Patil GP, Chitambar SD. Circulation of multiple Enterovirus serotypes causing hand, foot and mouth disease in India. J Med Microbiol 2012;61:420-5.
[Google Scholar]
|
| 6. |
Wei SH, Huang YP, Liu MC, Tsou TP, Lin HC, Lin TL, et al. An outbreak of coxsackievirus A6 hand, foot, and mouth disease associated with onychomadesis in Taiwan, 2010. BMC Infect Dis 2011;11:346.
[Google Scholar]
|
Fulltext Views
3,710
PDF downloads
2,163





![[Figure - 1]](#fig_ijdvl_2020_86_1_105_253985_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2020_86_1_105_253985_f2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2020_86_1_105_253985_f3.jpg){kind=link}