Translate this page into:
Happle-Tinschert syndrome: Report of a newly delineated entity
Correspondence Address:
Nayeem Sadath Haneef
7/202, Kalyani, Sahara States, LB Nagar, Hyderabad - 500 068, Andhra Pradesh
India
| How to cite this article: Haneef NS, Ramachandra S, Metta AK, Sushmalatha B, Bellam SS, Ohatkar N. Happle-Tinschert syndrome: Report of a newly delineated entity. Indian J Dermatol Venereol Leprol 2014;80:71-73 |
Sir,
Happle-Tinschert syndrome is a recently delineated multisystem birth defect of unknown etiology consisting of segmentally arranged basaloid follicular hamartomas associated with skeletal, dental and cerebral anomalies. [1],[2] In 2008, Happle and Tinschert of Germany reported these features in a 39-year-old man. They also reviewed eight similar cases reported by others under various designations and concluded that all those cases actually represent a spectrum of a distinct syndrome. [1] In 2009, Itin of Switzerland reported another typical case and proposed that this syndrome be named as "Happle-Tinschert syndrome." [2] Another case was reported by Boccaletti et al. of Italy in 2011. [3] We are reporting a similar case of Happle-Tinschert syndrome, which, to the best of our knowledge, is the first report of this new entity from Asia.
A 23-year-old woman presented with whitish streaks on the face, neck, left side of the trunk and left upper limb since birth. She developed asymptomatic, persistent, linearly arranged, raised, solid lesions within the whitish streaks since 12 years. There was no history of photosensitivity, abnormality of sweating, recurrent infections, visual impairment, hearing impairment, headache, convulsions, sensory or motor impairment, delayed milestones, consanguinity or family history of similar lesions.
Cutaneous examination revealed streaks of hypopigmented macules and atrophic areas along the Blaschko′s lines over face, neck, left side of upper trunk and left upper limb [Figure - 1]a and b. They were distributed bilaterally over face and neck but were present only on the left side of upper trunk and left upper limb with sharp midline demarcation indicating segmental distribution. Within these linear hypopigmented areas there were multiple, densely arranged and some scattered, skin colored to brownish, hairless papules, some having a comedo-like central plug [Figure - 2]a-c. Hypertrichosis and freckles were present over the face [Figure - 1]a. Palms, soles, mucosae and genitalia were normal.
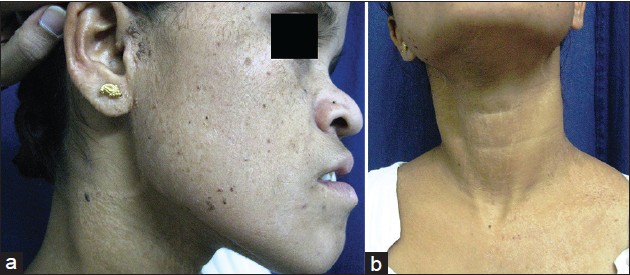 |
| Figure 1: (a) Blaschkoid hypopigmentation, atrophy, papules over face and neck with hypertrichosis, freckles and saddle nose (b) Hypopigmented, atrophic streaks and papules seen bilaterally over the neck and unilaterally over the trunk with sharp midline demarcation |
 |
| Figure 2: (a) Multiple, densely arranged and few scattered, skin coloured and brownish papules within linear hypopigmented areas over face (b) Brownish papules within hypopigmented, atrophic streaks in blaschkoid distribution over forearm (c) Skin colored and brownish black hairless papules with comedo-like central plug over the pre-auricular area |
General examination showed a depressed nasal bridge (saddle nose), hypertelorism and crowded teeth [Figure - 1]a. The left lower limb was 13 cm shorter than the right. There was an extra toe with dystrophic nail adjacent to left great toe (polydactyly) whereas right thumb was short and broad [Figure - 3]a and b. Her mental status was appropriate for her age. Abdominal, cardiovascular and respiratory system examination were normal.
 |
| Figure 3: (a) Short, broad right thumb (b) Polydactyly of left foot |
Histopathology of a papular lesion showed anastomosing strands of epidermal cells arising from the follicular infundibulum forming the characteristic "lattice pattern" [Figure - 4]a. The strands showed peripheral palisading of cells resembling basal cell carcinoma (BCC) [Figure - 4]b. Mitoses were very few. A comedo-like large pseudocyst was seen in the upper dermis. The dermal stroma was scanty. These features were diagnostic of basaloid follicular hamartoma. [1],[4],[5] There was no evidence of cervical rib on X-ray. Magnetic resonance imaging of the brain was normal.
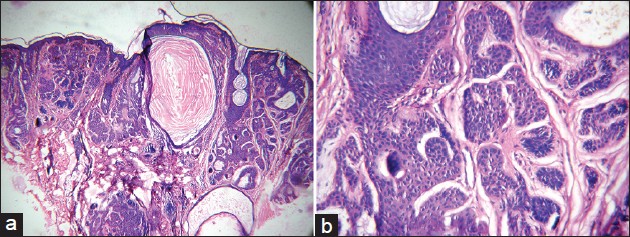 |
| Figure 4: (a) Histopathology of papule showing characteristic "lattice pattern" of anastomosing strands of epidermal cells and a comedo-like pseudocyst (H and E, ×10) (b) Peripheral palisading of cells but with very few mitoses suggestive of basaloid follicular hamartoma (H and E, ×40) |
In the differential diagnosis, generalized basaloid follicular hamartoma syndrome, Gorlin syndrome (naevoid BCC syndrome), Bazex Dupre-Christol syndrome, Apert′s syndrome, nevus comedonicus syndrome and familial multiple trichoepithelioma were considered. [1],[4],[6] Based on the segmental distribution of histopathologically confirmed basaloid follicular hamartomas and characteristic extracutaneous features, a diagnosis of "Happle-Tinschert syndrome" was made. After counseling about the disease, papular lesions were treated with electrocautery.
The cutaneous hallmark of Happle-Tinschert syndrome is segmental basaloid follicular hamartomas occurring along Blaschko′s lines, representing a mosaic phenotype. [1],[2] These benign neoplasms of the hair follicles may occur sporadically or in hereditary multiple basaloid follicular hamartomas, transmitted as an autosomal dominant trait. [5],[7] They manifest predominantly over the face as small, hairless, skin colored or brownish, persistent papules, some with a comedo-like central plug. [1],[5],[8] Histopathology shows characteristic "lattice-like pattern" of anastomosing strands of basaloid and squamoid cells proliferating downwards from the follicular infundibulum. [1],[4] Horn cysts can be seen and dermal stroma is scanty. [5] The basaloid cells in basaloid follicular hamartomas show less mitoses and single cell necroses compared to BCC. [7] Immunohistochemical staining for the proliferation markers ′proliferating cell nuclear antigen′ and ′Ki-67′ shows less staining in basaloid follicular hamartoma than in BCC. [7] Patched gene (PTCH) mutations are absent in blood deoxyribonucleic acid in basaloid follicular hamartoma unlike BCC. [1],[2] In the past, basaloid follicular hamartomas occurring in linear or segmental pattern have been reported and often misdiagnosed as nevus comedonicus syndrome or naevoid BCC syndrome (Gorlin′s syndrome). [1],[2],[9] In Happle-Tinschert syndrome, basaloid follicular hamartomas are densely arranged or scattered within segmentally distributed streaks of hypopigmentation and atrophy. [1],[2] Our case too showed similar lesions. Interestingly, the lesions were bilateral over face and neck but still showing blaschkoid pattern. Lesions of this syndrome should not be confused with generalized basaloid follicular hamartoma syndrome or other forms of nonsegmental basaloid follicular hamartomas. [1],[2]
Other cutaneous features seen in our patient were facial hypertrichosis and multiple freckles. Hypertrichosis or hypotrichosis, but not freckles, have been reported in previous cases of Happle-Tinschert syndrome. [1],[2] Other rarely reported cutaneous findings like palmoplantar pits, loose skin of hands and feet, webbing of toes, cutaneous and subcutaneous ossification and humped nasal bridge were absent in our patient. [1],[2]
Skeletal abnormalities in Happle-Tinschert syndrome are usually ipsilateral and include socket type or saddle nose, cervical rib, widening of paravertebral segments of ribs, scoliosis, deficient growth or overgrowth of the involved limb with muscular hyperplasia, pre-axial or post-axial polydactyly, malformed thumb and abnormal bone mineralization. [1],[2] Our patient also had saddle nose, short left lower limb with polydactyly (ipsilateral) and short, broad right thumb (contralateral) reminiscent of Apert′s syndrome. [10]
Previously reported ipsilateral dental abnormalities like enamel defects, anodontia, hypoplastic maxillary teeth or mandibular ameloblastoma were absent in our patient, but the teeth were crowded. Mental retardation and other central nervous system anomalies like enlarged third ventricle, optic glioma, meningioma, medulloblastoma or hemimegaloencephaly were not seen, though she may be at risk of developing these in the future. [1],[2],[3] Unconfirmed features of this syndrome like dysplastic ears, macroglossia, imperforate anus, cataract, microphthalmia, epicanthus, and conjunctival lipodermoid were absent, but she had hypertelorism, which has not been reported so far. [1],[2],[3]
In conclusion, Happle-Tinschert syndrome is a rare multisystem birth defect characterized by the cutaneous hallmark of segmental basaloid follicular hamartomas along with skeletal, cerebral, dental and ocular anomalies. Our case had most of these features along with hitherto undescribed features like bilateral occurrence of segmental basaloid follicular hamartomas, facial freckles and hyperteleorism.
| 1. |
Happle R, Tinschert S. Segmentally arranged basaloid follicular hamartomas with osseous, dental and cerebral anomalies: A distinct syndrome. Acta Derm Venereol 2008;88:382-7.
[Google Scholar]
|
| 2. |
Itin PH. Happle-Tinschert syndrome. Segmentally arranged basaloid follicular hamartomas, linear atrophoderma with hypo- and hyperpigmentation, enamel defects, ipsilateral hypertrichosis, and skeletal and cerebral anomalies. Dermatology 2009;218:221-5.
[Google Scholar]
|
| 3. |
Boccaletti V, Accorsi P, Pinelli L, Ungari M, Giordano L, Neri I, et al. Congenital systematized basaloid follicular hamartoma with microphthalmia and hemimegalencephaly. Pediatr Dermatol 2011;28:555-60.
[Google Scholar]
|
| 4. |
Mehregan AH, Baker S. Basaloid follicular hamartoma: Three cases with localized and systematized unilateral lesions. J Cutan Pathol 1985;12:55-65.
[Google Scholar]
|
| 5. |
Brownstein MH. Basaloid follicular hamartoma: Solitary and multiple types. J Am Acad Dermatol 1992;27:237-40.
[Google Scholar]
|
| 6. |
Happle R. The group of epidermal nevus syndromes Part I. Well defined phenotypes. J Am Acad Dermatol 2010;63:1-22;23.
[Google Scholar]
|
| 7. |
Jih DM, Shapiro M, James WD, Levin M, Gelfand J, Williams PT, et al. Familial basaloid follicular hamartoma: Lesional characterization and review of the literature. Am J Dermatopathol 2003;25:130-7.
[Google Scholar]
|
| 8. |
Girardi M, Federman GL, McNiff JM. Familial multiple basaloid follicular hamartomas: A report of two affected sisters. Pediatr Dermatol 1999;16:281-4.
[Google Scholar]
|
| 9. |
Jiménez-Acosta FJ, Redondo E, Baez O, Hernandez B. Linear unilateral basaloid follicular hamartoma. J Am Acad Dermatol 1992;27:316-9.
[Google Scholar]
|
| 10. |
Yaghoobi R, Bagherani N, Tajalli M, Paziar N. Apert syndrome. Indian J Dermatol Venereol Leprol 2010;76:724.
[Google Scholar]
|
Fulltext Views
3,683
PDF downloads
3,534





![[Figure - 1]](#fig_ijdvl_2014_80_1_71_125468_u1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2014_80_1_71_125468_u2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2014_80_1_71_125468_u3.jpg){kind=link}
![[Figure - 4]](#fig_ijdvl_2014_80_1_71_125468_u4.jpg){kind=link}