Translate this page into:
Innovations in dermatology
Correspondence Address:
C R Srinivas
Department of Dermatology, Venereology and STD, PSG Institute of Medical Sciences and Research, Coimbatore, Tamil Nadu
India
| How to cite this article: Srinivas C R. Innovations in dermatology. Indian J Dermatol Venereol Leprol 2016;82:641-644 |
“There is a better way to do it, find it.”
Innovation is an outcome of wanting to improvise, not accepting anything as the final word written or said. After one of my presentations, I was asked, “But are you not reinventing the wheel?” I replied, “Yes, but had the wheel not been improved again and again, we will still be rolling on logs.”
An idea, especially solutions to a long-vexing problem pops up suddenly and in a rush. Adrenalin rushes in and there is a thrill to it which is akin to rapid descent from heights. It is no respecter of time or place. Archimedes got it in the bathtub. Now, not everyone in a bathtub will get the idea although all will displace water. He got it because he had parked the question at his subconscious level and unknowingly at all times and at all places he was seeking the answer. He was both obsessed with the problem and passionate about finding a solution. Before he struck gold, he must have worked on many explanations which he would have analyzed and rejected.
Our mind is conditioned like Pavlov's canine friends. We see all leaves as green because we have been told that leaves have chlorophyll and it is a green pigment and so all leaves are green but the fact is leaves are rarely just green, and at times not green at all. We hesitate to see or say what we see, lest we become an object of ridicule. We see the King well attired when he is, in fact, nude. Peer approval is foremost in our mind. To think out of the box, peer pressure should not matter. One should be a non-conformist. One should question, seek explanations for every single day-to-day occurrence which is taken for granted.
Everyone knew that an apple, when it falls, would land on the ground. Newton asked why and rest is history. He asked the right question. To innovate one should ask the right question.
In our dermatology practice, we see numerous conditions. Many are either due to or are altered by physical or chemical causes. Candidal intertrigo between the toes maybe due to fungus but treating for fungus alone will not cure the condition. Physical factors such as heat, moisture and lack of aeration are other factors which need to be addressed. Now these requirements were parked in the subconscious level. During ACSICON at Mahabaleshwar, the best paper award went to a metallic toe separator which is unlikely to be comfortable. I had advised hair bands which can be worn on the toes like rings, but no one would either search for it or buy it. Freshly back from conference, I was at my clinic when a patient with intertrigo between toes came for treatment. I had just finished a procedure and adhesive stretchable tape was in front of me. In a flash, an idea came and a toe separator overcoming the above-mentioned disadvantage was assembled [Figure - 1],[Figure - 2],[Figure - 3]. This highlights the fact that innovative ideas come only if one is very much involved in the subject.
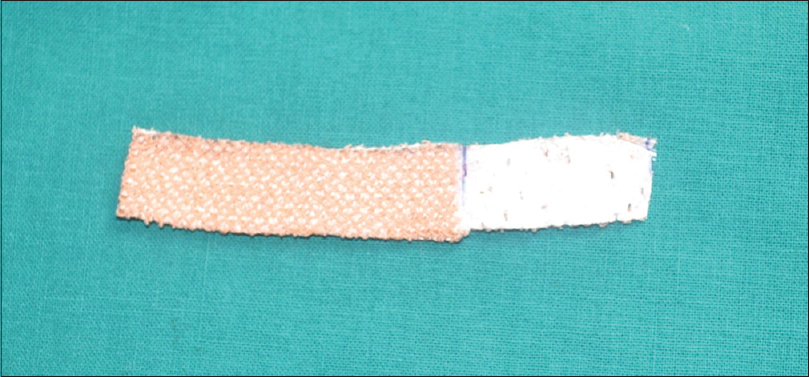 |
| Figure 1: Adhesive stretchable plaster folded upon itself |
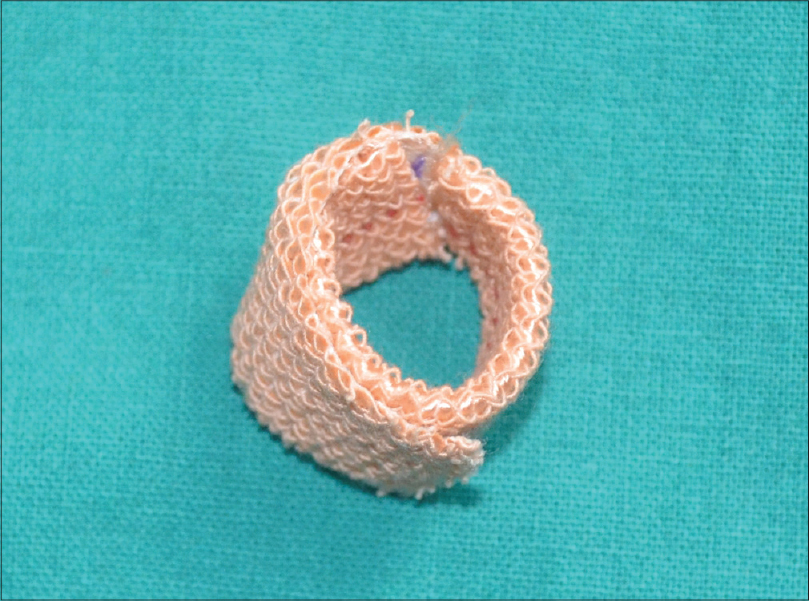 |
| Figure 2: Toe separator |
 |
| Figure 3: Wider interdigital space |
Innovative ideas are like brainstorming. During brainstorming, one records all suggestions, even the most impractical ones. Likewise, if an idea comes it should not be rejected off hand. It should be noted down and explored. The idea is then tested by conveying it to another person in the same or related field over coffee or beer. Sharing of vaguely formed ideas should be for organizing the idea in one's own mind and getting the syntax right. While explaining to someone, shortcomings will become evident and course correction can be undertaken. On occasions, the idea can be placed in cold storage. One can ask the other person to carry forward the idea and life is easier if issue of copyright is not worried about. In my experience, though, only rarely will a third person carry out the study until the end. Most ideas die if passed on and not pursued by the originator.
Innovations are often needed. It is determined by what the situation demands. It requires understanding the situation. It calls for dismantling the entire object into smaller parts, comprehending and appreciating the importance of the part for the whole. Tweaking the part and then replacing the tweaked part.
Let me share an example. We see many cases of toxic epidermal necrolysis due to drugs. The management of this condition has multiple arms. Now, each arm should be worked upon as a separate issue. Let us take the issue of skin fragility and how it sticks to clothing and dressing. We use banana leaf as a non-adhesive dressing. However, many patients on treatment develop infection. Can the leaf be one of the contributing factors? Can this be proved? If yes, how? If proved, can such transmission be prevented? Moreover, these questions resulted in our innovative use of sterilized banana leaf.[1] Similarly, we addressed temperature regulation and foul odor and we addressed these by the use of cradle or hood and the use of activated charcoal.[2],[3] We did not tinker with drugs and fluid replacement which is also part of the whole but were not addressed during the study.
Let me share some other examples. Pull test for hair loss is a useful test but lacks standardization. Can it be standardized? This resulted in the development of trichotillometer, a device used to measure the force needed to pluck hair [Figure - 4]. Innovations are needed to save money and increase the use of available resource. Antigens for patch testing are expensive. It is difficult to procure all series since patients needing the test will be few and far between. We devised a method using what is available to preload the chambers for testing and posting the same to another center which can test with the antigens without having to invest a huge amount to buy the entire series.[4] The story of the evolution of bath suit in place of bathtub to deliver psoralen for psoralen and ultraviolet A (PUVA)/PUVAsol is somewhat similar.[5] It addressed the difference in living style in India where bathtub is not installed at most houses.
 |
| Figure 4: Trichotillometer |
Yet, another approach which could result in innovation is to exploit an unwanted effect. If one man's meat can be another man's poison then what is a side effect in one situation can be a treatment in another. Botox and minoxidil are glaring examples. Poison, if carefully and imaginatively handled, can become a medicine. One such innovative use is the use of triple combination. Kligman possibly did a great disservice by advocating the formulation for use on face for pigmentation but it seems to work for postinflammatory pigmentation on legs following lichen planus and also in Kyrle's disease although this avatar needs confirmation by further studies. Hydroquinone addresses the pigmentation, retinoids, the dyskeratosis and topical steroids, suppress inflammation and relieve itching.
Till now, I have been discussing how to innovate in general, and dermatology in particular. An innovator does not respect boundaries and walls are there to be scaled. He often skates on thin ice.
Innovation can also extend to our conferences. Most of us will agree that we have conferences one too many and many are repetitive. Delegates find stalls more amusing and are affectionately referred to as stalwarts. Some like to see places nearby and far. Scientific hall remains empty. An innovator will ask why this is happening and then he will try and provide drama, action and screenplay intermixed with dermatology during the Congress thereby forcing delegates to think twice before leaving the venue. One of the best ways to make a person feel small is to look in his eyes and say, “Oh boy, did you miss something,” and walk away whereas the absentee swells when he is told, “You missed nothing.” Subject was the same, same old contact dermatitis and chemical peels but has been innovatively packaged as, “Point counter Point” and “Coffee with Maya.” We experimented with this at Coimbatore and the result was heartening.
Innovations really help in learning and can be attempted in many ways in dermatology. Use of social media for learning is in itself an innovation and provides unlimited scope and opportunity. Discipline in the department too can be enforced without having to issue threats. The university has ruled that students should continue to attend classes and attend to duty until the last date of the course even if the final postgraduate examinations have been conducted and results possibly unofficially known. However, the students were almost always irregular and chose to attend at will. It was then decided that the number of days these students failed to attend will be deducted from the unofficial study holidays of the next examination going batch and absenteeism reduced dramatically! Innovations need spiral thinking and at times a convoluted thought process when a straightforward approach fails to pay dividends.
To conclude, innovation is the way forward. It does not demand great intelligence but the ability to ask the right questions at the right time, belief in oneself, communication skills and madness in small, yet acceptable quantities.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
| 1. |
Srinivas CR, Sundaram VS, Raju BA, Prabhu SK, Thirumurthy M, Bhaskar AC. Achieving asepsis of banana leaves for the management of toxic epidermal necrolysis. Indian J Dermatol Venereol Leprol 2006;72:201-2.
[Google Scholar]
|
| 2. |
Prabhu KS, Srinivas CR, Nair S, Sundaram SV, Thirumurthy M. Exploiting the igloo principle and greenhouse effect to regulate humidity and temperature. Indian J Dermatol Venereol Leprol 2006;72:361-3.
[Google Scholar]
|
| 3. |
Chakravarthi A, Srinivas CR, Mathew AC. Activated charcoal and baking soda to reduce odor associated with extensive blistering disorders. Indian J Dermatol Venereol Leprol 2008;74:122-4.
[Google Scholar]
|
| 4. |
Chakravarthi SR. Transporting preloaded chambers for patch testing. Indian Dermatol Online J 2012;3:57-8.
[Google Scholar]
|
| 5. |
Pai S, Srinivas CR. Bathing suit delivery of 8-methoxypsoralen for psoriasis: A double-blind, placebo-controlled study. Int J Dermatol 1994;33:576-8.
[Google Scholar]
|
Fulltext Views
4,747
PDF downloads
2,478





![[Figure - 1]](#fig_ijdvl_2016_82_6_641_190871_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2016_82_6_641_190871_f2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2016_82_6_641_190871_f3.jpg){kind=link}
![[Figure - 4]](#fig_ijdvl_2016_82_6_641_190871_f4.jpg){kind=link}