Translate this page into:
Lethal melanoma in a two-year-old child with multiple congenital melanocytic nevi
Correspondence Address:
Linlin Xin
16766 Jingshi Rd, Jinan, Shandong 250014
China
| How to cite this article: Gao F, Niu G, Zhang B, Xin L. Lethal melanoma in a two-year-old child with multiple congenital melanocytic nevi. Indian J Dermatol Venereol Leprol 2019;85:89-93 |
Sir,
Pediatric melanoma is rare, accounting for only 1–4% of all cases of melanoma and 1–3% of all pediatric malignancies.[1] Here we describe a rare case of malignant melanoma in a two-year-old boy with multiple congenital melanocytic nevi. This case of melanoma showed rapid progression, metastasis and eventual death.
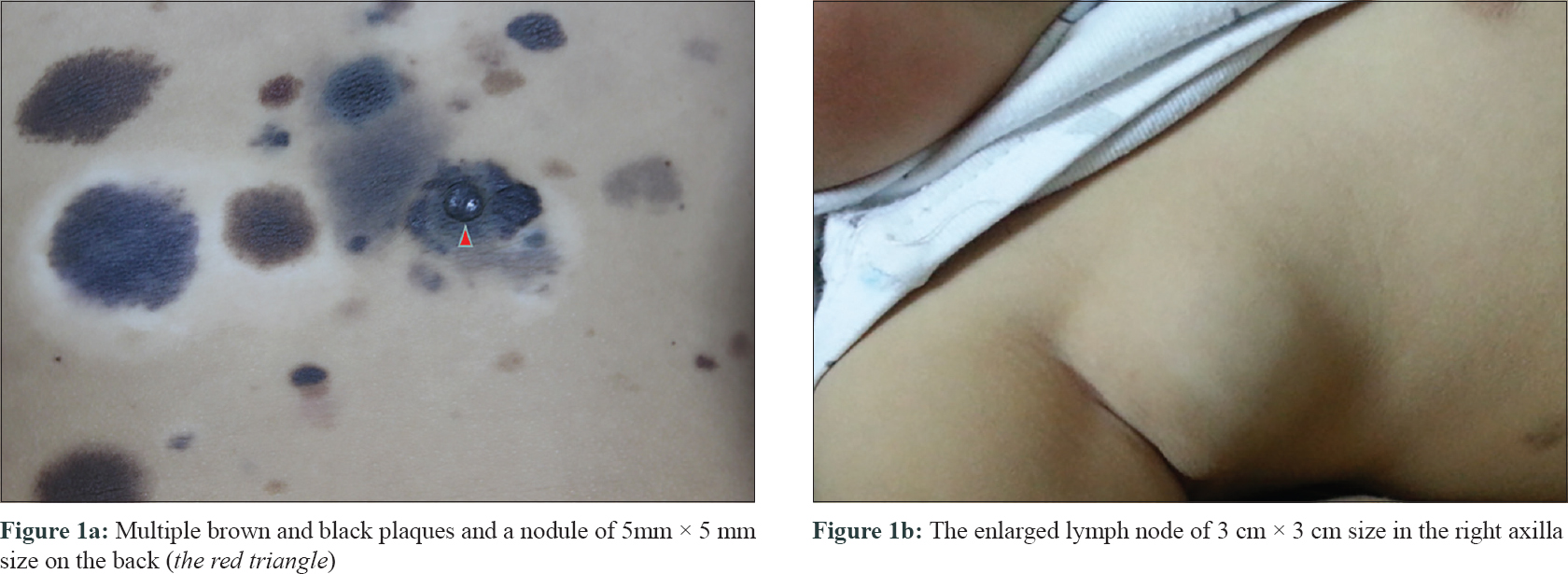
A 2 -year-old boy presented with multiple brown and black lesions on the back noticed since birth. It was noted that all lesions were flat and did not show changes until 10 months of age. This child was born out of a non-consanguineous marriage by normal vaginal delivery at term. There was no history of trauma or infection. There was no family history of melanoma or other malignancies. Examination revealed multiple hyperpigmented plaques of size varying from 0.5 cm to 3 cm. The plaques were mainly distributed on the back but some smaller ones were also found on the subcostal region of right flank. In total, lesions and satellites covered approximately 6% of body surface area. Face, chest, abdomen and limbs were spared. One of the plaques on the back was studded with a nodule of 5 mm × 5 mm size [Figure - 1]a.
 |
| Figure 1 |
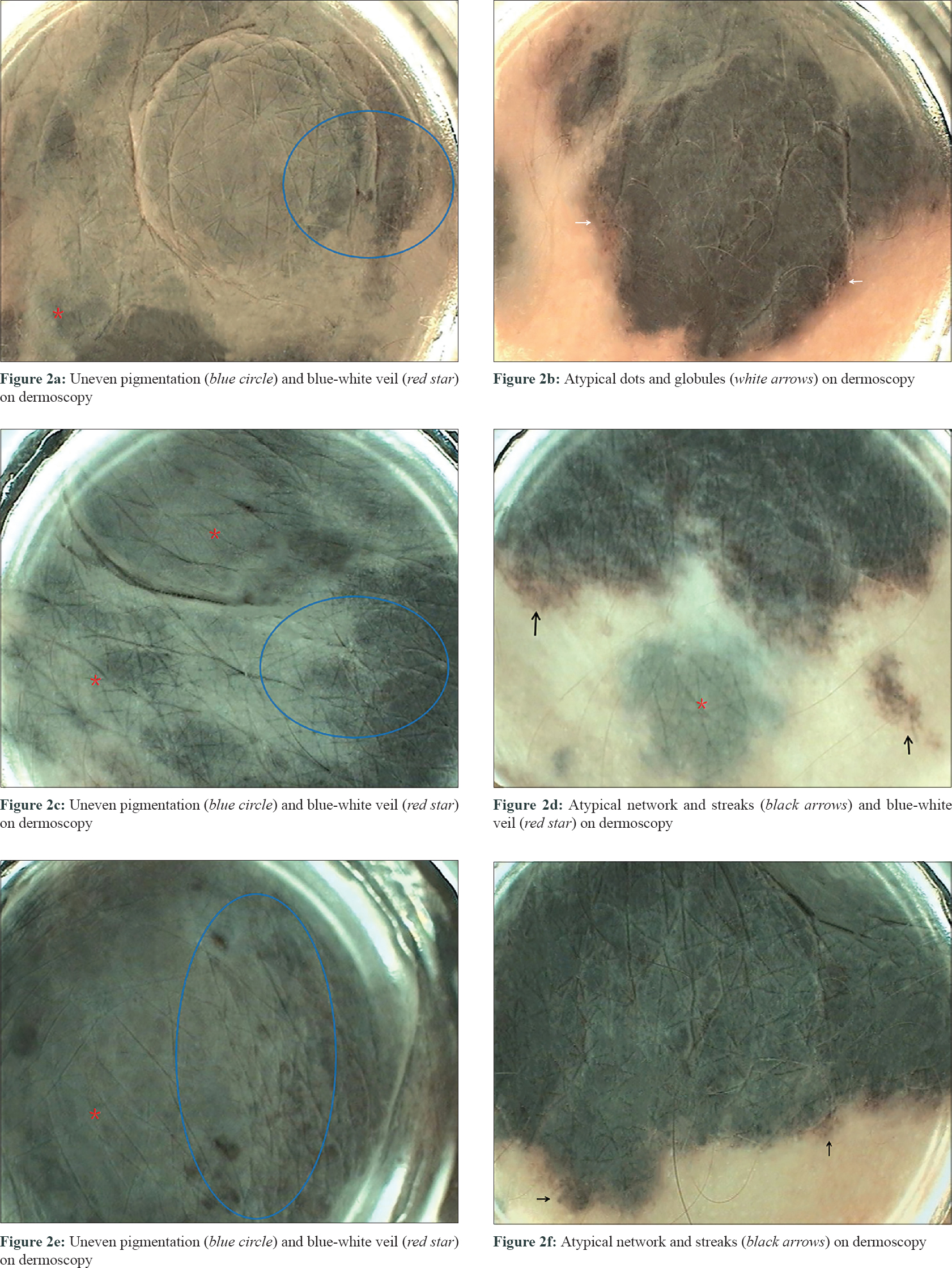
Dermoscopy of the nodule on the back revealed incomplete pigmentation, blue-and-white veil [Figure - 2]a, [Figure - 2]c and [Figure - 2]e, atypical dots and globules [Figure - 2]b and atypical reticular formations and striae [Figure - 2]d and [Figure - 2]f, showing features of malignant melanoma.
 |
| Figure 2 |
Parents did not consent for a skin biopsy. Follow-up visits were advised every 3 months so that the lesions could be monitored through dermoscopy.
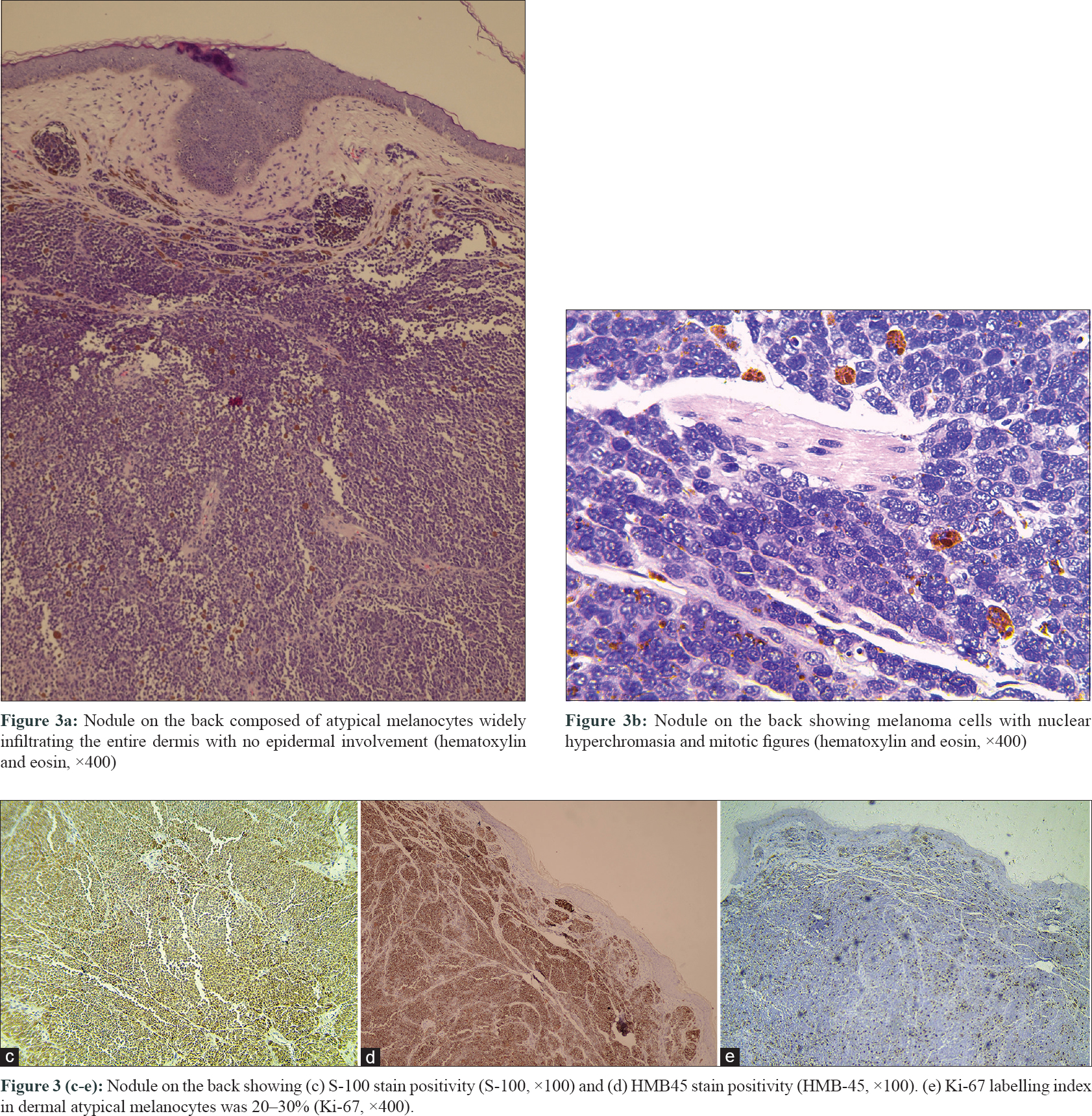
Nine months later, parents agreed for a skin biopsy. Biopsy was done from the nodule arising from a hyperpigmented plaque on the back. Histopathologically, the tumor was composed of atypical melanocytes infiltrating the entire dermis extensively without any epidermal involvement [Figure - 3]a. It was shown that the melanocytes had nuclear hyperchromasia. Mitotic figures could also be observed [Figure - 3]b. Two mitotic figures were observed per 10 high power regions. The thickness of the tumor (Breslow) was 7 mm, the Clark level was IV and the tumor stage was evaluated as IIIB. The immunohistochemical examination revealed that atypical melanocytes were positive for S-100 [Figure - 3]c and HMB-45 [Figure - 3]d. The Ki-67 labelling index in dermal atypical melanocytes was 20–30% [Figure - 3]e. Both HMB45 and Ki-67 positivity of melanocytes in deep dermis were highly suspicious of malignant transformation.
 |
| Figure 3 |
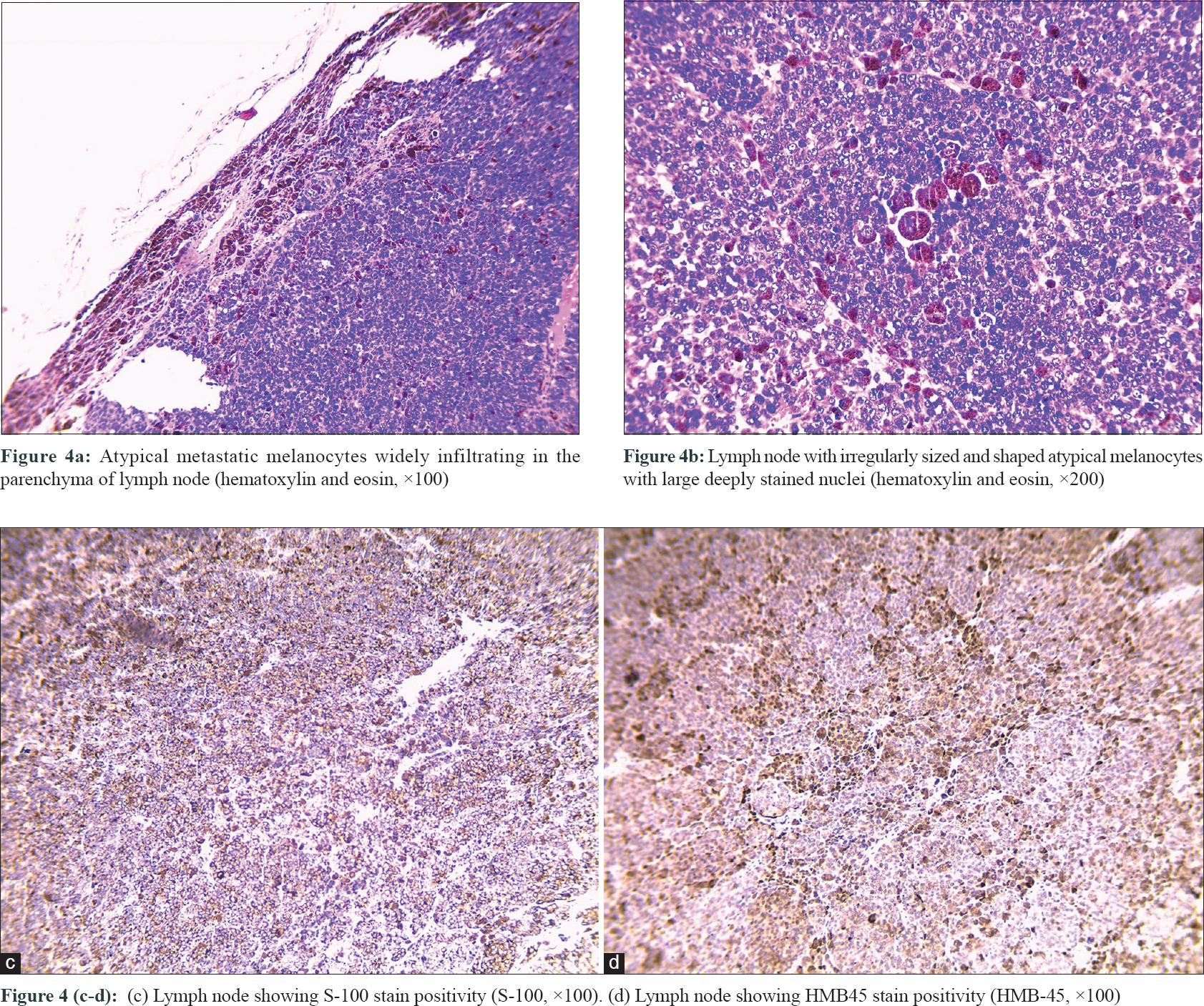
After 4 months the child presented with a 3 cm × 3 cm tumor on the right axilla. Lymph node metastasis was clinically suspected [Figure - 1]b. Histopathological examination revealed atypical metastatic melanocytes with deep staining of the nucleus and melanin extensively infiltrating lymph node parenchyma [Figure - 4]a and [Figure - 4]b. Immunohistochemical examination showed positive staining for S-100 and HMB45 [Figure - 4]c and [Figure - 4]d. This case was diagnosed as malignant melanoma arising from a congenital melanocytic nevus with lymph node metastasis.
 |
| Figure 4 |
The child did not receive any computed tomography scans or treatment due to financial constraint. The child died a year after the initial diagnosis. It was informed that the boy was in a coma during the last months of his life. Therefore, it is speculated that he might have developed widespread metastases involving the brain as well. Brain metastasis often occurs when a tumor is located near the spine.
The biggest challenge in diagnosis is to distinguish between melanomas arising from congenital melanocytic nevus and proliferating nodules that develop in congenital melanocytic nevus. There are several features that distinguish between proliferating nodule and melanoma: (1) lack of highly uniform cell atypicality; (2) lack of necrosis within the nodule; (3) rarity of mitosis; (4) evidence of maturation of cells in a mixed or transitional form; (5) lack of spread into the epidermis and (6) absence of destructive bloated growth.[1]
It is generally accepted that a complete excision in early childhood decreases the risk of malignancy[2]. Another option is a close monitoring by physical examination, including lymph node palpation and dermoscopy, with periodic follow-up and prompt excision if the lesion presents variations.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the parents have given their consent for images and other clinical information to be reported in the journal. The parents understand that names and initials will not be published and due efforts will be made to conceal patient identity, but anonymity cannot be guaranteed.
We have obtained all appropriate patient consent forms.
Financial support and sponsorship
Shandong Province Science and Technology Development Project (2013GSF11835).
Conflicts of interest
There are no conflicts of interest.
| 1. |
Xu X, Bellucci KS, Elenitsas R, Elder DE. Cellular nodules in congenital pattern nevi. J Cutan Pathol 2004;31:153-9.
[Google Scholar]
|
| 2. |
Cordoro KM, Gupta D, Frieden IJ, McCalmont T, Kashani-Sabet M. Pediatric melanoma: results of a large cohort study and proposal for modified ABCD detection criteria for children. J Am Acad Dermatol. 2013; 68:913-25.
[Google Scholar]
|
Fulltext Views
2,813
PDF downloads
2,607





![[Figure - 1]](#fig_ijdvl_2019_85_1_89_247780_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2019_85_1_89_247780_f2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2019_85_1_89_247780_f3.jpg){kind=link}
![[Figure - 4]](#fig_ijdvl_2019_85_1_89_247780_f4.jpg){kind=link}