Translate this page into:
Leukemia cutis following herpes zoster infection: An unusual example of Wolf's isotopic response
2 Department of Dermatology, The First Affiliated Hospital of Fujian Medical University; Department of Dermatology, Dermatology Hospital of Fuzhou, Fuzhou, Fujian, China
3 Midwest Center for Dermatology, Clinton, Michigan, US
Correspondence Address:
Hui-Chun Su
Department of Dermatology, The First Affiliated Hospital of Fujian Medical University, 20 Chazhong Road, Taijiang District, Fuzhou, Fujian 350004
China
| How to cite this article: Ke H, Gong XP, Su HC, Su W, Cheng B. Leukemia cutis following herpes zoster infection: An unusual example of Wolf's isotopic response. Indian J Dermatol Venereol Leprol 2019;85:539-541 |
Sir,
Wolf's isotopic response designates the appearance of a new dermatosis at the site of an already healed unrelated skin disease. The initial dermatosis is usually a herpetic infection, particularly herpes zoster.[1] It acts as a presumed trigger for local immune dysregulation, resulting in the development of subsequent skin lesion.
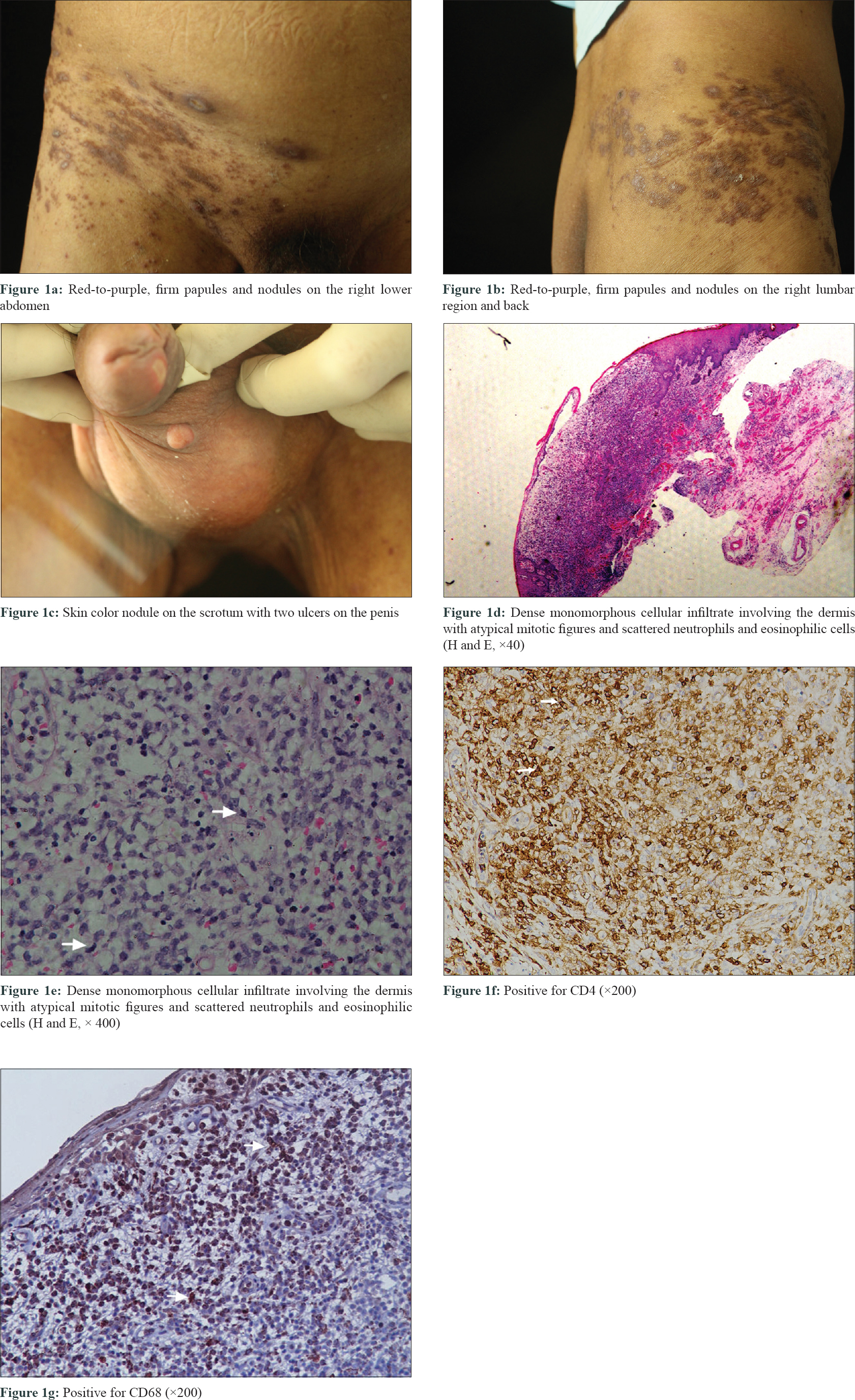
A 68-year-old man presented to us with sudden eruption of clustered, painful vesicles and erythema on his right lumbar region (L1–L4), suggestive of herpes zoster. He was a known case of acute monocytic leukemia (AML-M5), failing to achieve complete clinical remission despite receiving several chemotherapy cycles containing homoharringtonine (omacetaxine mepesuccinate) and cytarabine since last 2 years. He received 0.5 g of intravenous acyclovir every 8 h for 14 days for his presenting complaint. The lesions healed with residual \postinflammatory hyperpigmentation. After 10 days, red-to-purple, firm, spontaneously painful papules and nodules appeared on the healed area; without any vesicle. [Figure - 1]a, [Figure - 1]b, [Figure - 1]c. Additionally, a skin coloured nodule developed on the scrotum along with two penile ulcers. He was administered 0.5mg methylcobalamin (IV) and oral pregabalin 75 mg twice daily for presumed zoster-related neural pain. His total leukocyte count was 24.72 × 10(9)/L (3.5 ~ 9.5 × 10(9)/L), monocyte count 0.87 × 10(9)/L (0.1 ~ 0.6 × 10(9)/L), red blood cell count 2.07 × 10(12)/L (3.8 ~ 5.1 × 10(12)/L), haemoglobin 63 g/L (115 ~ 150 g/L), and platelet count 11 × 10(9)/L (125 ~ 350 × 10(9)/L) on routine blood biochemistry. He received 2.8 units of platelet transfusion for thrombocytopenia. Skin biopsies of the truncal and left scrotal nodules demonstrated a dense monomorphous, mononuclear, cellular infiltrate in the dermis with blast morphology and atypical mitotic figures. Scattered neutrophilic and eosinophils cells were also observed. [Figure - 1]d and [Figure - 1]e. The immunohistochemical staining demonstrated positive results for lysozyme, CD68, CD43, and CD4 [Figure - 1]f and [Figure - 1]g, but terminal deoxynucleotidyl transferase (TDT), CD117, and Epstein-Barr virus encoded small RNA (EBER) were negative. 40% cells showed a positive staining with Ki67. Based on this a diagnosis of leukemia cutis developing as a Wolf's isotopic response following herpes zoster, in a case of treatment-refractory AML was made. The patient refused to take the recommended specific therapy. Unfortunately, we lost the patient to a bleeding episode caused by thrombocytopenia within 1 month.
 |
| Figure 1 |
The term “Wolf's isotopic response” describes the occurrence of a new skin condition at the same location of a healed, unrelated dermatosis. Granulomatous reactions, malignant infiltrates, lichenoid dermatitis, or infections are the most common isotopic responses, which appear days or years after the initial disease has healed.[2] Many etiopathogenic mechanisms have been proposed including viral, neural, vascular, and immunologic factors. Although localised immunological imbalance is considered to be the major contributory factor, the exact pathogenesis is still unclear. In our case, leukemia cutis occurred at the site of healed herpes zoster, so we are considering it as a Wolf's isotopic response.
Leukemia cutis occurs in 2%–3% of patientswithacute myelocytic leukemia.[3] Skin infiltration in AML-M5 has a poor prognosis, and most patients die within 1 year following diagnosis.[4] Leukemic infiltration occurring as a consequence of isotopic response is a rare event. We were unable to find any previous reports of acute myeloid leukemia skin infiltration presenting as Wolf's isotopic response. We considered herpes zoster–like metastases, infectious granuloma, and hypertrophic scar as the possible differential diagnoses.
In a series of nine patients with Wolf's isotopic response, two cases of B-cell chronic lymphocytic leukemia and one case of non-Hodgkin's lymphoma were reported following herpes zoster. Out of nine cases of B-cell chronic lymphocytic leukemia following a herpetic infection, seven experienced resolutions of cutaneous lesions without the worsening of the clinical prognosis, while two had poor outcomes.[5]
Leukemia cutis has protean cutaneous manifestations resulting in diagnostic dilemmas. Thus, we need a high index of suspicion to perform a prompt skin biopsy to prevent diagnostic delay. We should not confuse leukemic cutis with relapse of previously diagnosed and treated dermatitis, especially in the scenario of isotopic response.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patient has given his consent for his images and other clinical information to be reported in the journal. The patient understands that name and initials will not be published and due efforts will be made to conceal identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
| 1. |
Wolf R, Wolf D, Ruocco E, Brunetti G, Ruocco V. Wolf's isotopic response. Clin Dermatol 2011;29:237-40.
[Google Scholar]
|
| 2. |
Mehra T, Metzler G, Bauer J, Köberle M, Garbe C. Isotopic response of graft versus host disease following herpes zoster infection: Case report and review of the literature. Acta Derm Venereol 2012;92:383-4.
[Google Scholar]
|
| 3. |
Cronin DM, George TI, Sundram UN. An updated approach to the diagnosis of myeloid leukemia cutis. Am J Clin Pathol 2009;132:101-10.
[Google Scholar]
|
| 4. |
Jin X, Li F, Li X, Zhu W, Mou Y, Huang Y, et al. Cutaneous presentation preceding acute monocytic leukemia: A CARE-compliant article. Medicine (Baltimore) 2017;96:e62-9.
[Google Scholar]
|
| 5. |
Jaka-Moreno A, López-Pestaña A, López-Núñez M, Ormaechea-Pérez N, Vildosola-Esturo S, Tuneu-Valls A, et al. Wolf's isotopic response: A series of 9 cases. Actas Dermosifiliogr 2012;103:798-805.
[Google Scholar]
|
Fulltext Views
3,590
PDF downloads
2,092





![[Figure - 1]](#fig_ijdvl_2019_85_5_539_264105_f1.jpg){kind=link}