Translate this page into:
Linear cutaneous lupus erythematosus
2 Department of Pathology, Ramon y Cajal Hospital, Madrid, Spain
Correspondence Address:
Javier Alc�ntara-Gonz�lez
Department of Dermatology, Ram�n y Cajal Hospital, Madrid
Spain
| How to cite this article: Alc�ntara-Gonz�lez J, Fernandez-Guarino M, Carrillo-Gijon R, Ja�n-Olasolo P. Linear cutaneous lupus erythematosus. Indian J Dermatol Venereol Leprol 2011;77:717-719 |
Sir,
Linear lesions following the lines of Blaschko of discoid lupus erythematosus (DLE), subacute cutaneous lupus erythematosus or tumid lupus erythematosus are called linear cutaneous lupus erythematosus (LCLE). LCLE is a highly unusual variant of cutaneous lupus. It occurs mainly in children and young adults with a similar incidence in both sexes, and photosensitivity is less frequent. Lesions appear as linear unilateral erythematous plaques and predominate in the face; however, neck, trunk or the extremities may also be affected. In the majority of the cases, lesions are restricted to one anatomical site, and only one 8-year old boy showed widespread DLE to our best knowledge in literature search. [1] We report two cases of adult patients (≥15 years old) with LCLE. To our knowledge, there are only 10 previous reports of LCLE in adults.
A 64-year-old male with a previous medical history significant for ankylosing spondylitis was referred because of a 7 month history of a persisting asymptomatic linear erythematus lesion on the right side of his neck. No history of preceding trauma or exposure to sunlight was present. The lesion showed follicular plugging [Figure - 1]a. The results of routine laboratory tests were normal and antinuclear antibodies (ANAs) were absent. Histological examination revealed orthokeratotic hyperkeratosis with keratotic plaques and liquefaction degeneration of the dermo-epidermal junction. Dense mononuclear infiltrates around perivascular and periadnexal areas were seen in the dermis [Figure - 2]a. Mucin could also be observed in the dermis with colloidal iron stain [Figure - 2]b. Topical mometasone 0.1% cream was recommended twice daily which resulted in complete resolution of the lesion after two months [Figure - 1]b.
 |
| Figure 1: a: Erythematous linear plaques with follicular plugging on the right side of the neck of the first patient in the study Figure 1: b: Complete resolution of the lesion after treatment with topical corticosteroids of the first patient in the study |
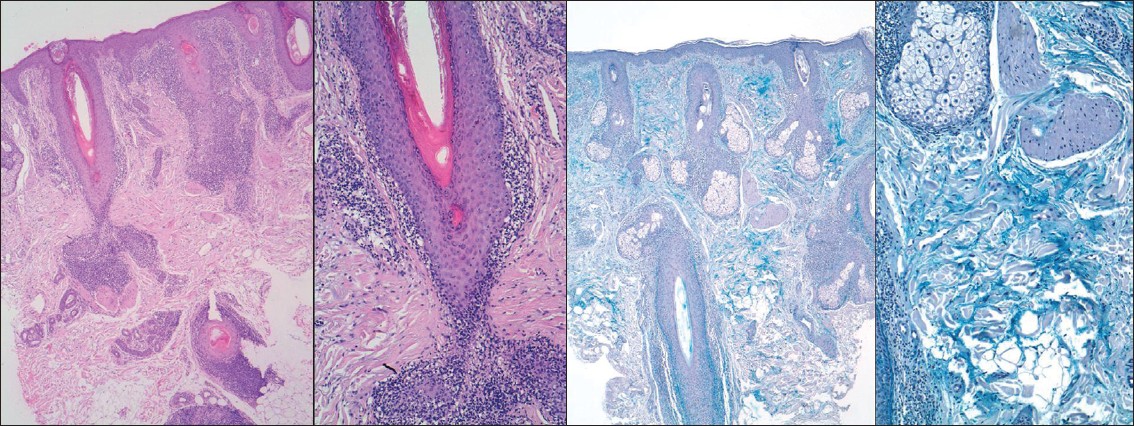 |
| Figure 2: a: Orthokeratotic hyperkeratosis, liquefaction degeneration of the dermo-epidermal junction and dense mononuclear infiltrates around perivascular and periadnexal areas during histological examination of the lesion of the first patient in the study (H and E, ×4 and ×20) Figure 2: b: Mucin deposits in dermis during histological examination of the lesion of the first patient in the study (colloidal iron stain, ×4 and ×20) |
A 45-year-old male presented with a several months history of enlarging, linear erythematous plaques with alopecia following the lines of Blaschko on the scalp [Figure - 3]. His medical history was unremarkable. Routine laboratory tests were normal, and ANAs were also absent. A biopsy specimen showed superficial and deep perivascular dermatitis with mild orthokeratotic hyperkeratosis, follicular plugging, vacuolar basal cell degeneration, mild exocytosis and dense mononuclear infiltrates around periadnexal areas. A residual scar remained after treatment which was treated with topical mometasone 0.1% cream twice daily for three months.
 |
| Figure 3: Erythematous linear plaques with alopecia on the scalp of the second patient in the study |
The lines of Blaschko were first described in 1901; however, their origin still remains unknown. They are believed to represent the developmental growth pattern of the embryonic ectodermal cells; and therefore, cutaneous lesions of LCLE would reflect the distribution of clones of abnormal keratinocytes arising during embryogenesis. Another theory suggests that these lines are the consequence of the expression of foreign antigens on involved cells, possibly caused by a genetic mosaicism. [2]
To our knowledge, less than 25 cases of LCLE have been reported in English and Spanish literature (15 children and 9 adults). [2],[3] Lesions of DLE were the most frequently found in cases of LCLE; however, lesions of cutaneous lupus erythematosus or tumid lupus have also been seen. Diagnosis of LCLE is made according to the clinical presentation and histopathological results. In most of these patients, testing for autoantibodies was negative (in 7 of 9 adult patients); however, direct immunofluorescence (DIF) was positive in 5 of 9 adult patients. [2],[3] Though DIF is not essential for the diagnosis of cutaneous lupus erythematosus, it is useful in cases where histology is not conclusive. In our cases, histological findings were so characteristic (hyperkeratosis, vacuolar basal cell degeneration, follicular plugging, lymphocytic infiltrates in a perivascular and periadnexal location and abundance of mucin within the dermis) that DIF was considered not necessary for the diagnosis. Differential diagnosis must be established with other conditions with Blaschkolinear distribution such as linear lichen planus, lichen striatus, linear granuloma annulare, linear psoriasis, morphea or inflammatory linear verrucous epidermal nevus. Systemic involvement has not been previously reported in LCLE; however, association with submandibular myoephitelial sialadenitis and localized scleroderma was seen in two cases. [4],[5]
Several treatments have been used including topical corticosteroids or systemic treatments such as hydroxychloroquine or dapsone. Improvement or complete resolution was obtained in most cases.
| 1. |
Green JJ, Baker DJ. Linear childhood discoid lupus erythematosus following the lines of Blaschko: A case report with review of the linear manifestations of lupus erythematosus. Pediatr Dermatol 1999;16:128-33.
[Google Scholar]
|
| 2. |
Thind CK, Husain EA, Hewitt J. A rare linear atrophic lesion on the face. Clin Exp Dermatol 2009;34:e447-8.
[Google Scholar]
|
| 3. |
Gaitanis G, Nomikos K, Chaniotakis I, Stergiopoulou C, Zioga A, Bassukas I. Linear cutaneous lupus erythematosus: A subset of childhood cutaneous lupus erythematosus. Lupus 2009;18:759-61.
[Google Scholar]
|
| 4. |
Davies MG, Newman P. Linear cutaneous lupus erythematosus in association with ipsilateral submandibular myoepithelial sialadenitis. Clin Exp Dermatol 2001;26:56-8.
[Google Scholar]
|
| 5. |
Umbert P, Winkelmann RK. Concurrent localized scleroderma and discoid lupus erythematosus: Cutaneous 'mixed' or 'overlap' syndrome. Arch Dermatol 1978;114:1473-8.
[Google Scholar]
|
Fulltext Views
5,684
PDF downloads
1,745





![[Figure - 1]](#fig_ijdvl_2011_77_6_717_86497_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2011_77_6_717_86497_f2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2011_77_6_717_86497_f3.jpg){kind=link}