
Translate this page into:
Linezolid: A novel treatment option for the treatment of a non-responsive case of actinomycotic mycetoma
Corresponding author: Dr. Neetu Bhari, Department of Dermatology and Venereology, All India Institute of Medical Sciences, Room No. 4070, 4th Floor Teaching Block, Ansari Nagar, New Delhi - 110 029, India. drntbhari@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Patra S, Senthilnathan G, Ramam M, Arava S, Bhari N. Linezolid: A novel treatment option for treatment non-responsive case of actinomycotic mycetoma. Indian J Dermatol Venereol Leprol 2021;87:455.
Sir,
Linezolid, an oxazolidinone antibiotic, is commonly used in the management of skin and soft tissue infections caused by Gram-positive bacteria, primarily, methicillin-resistant Staphylococcus aureus.1 Recent studies have shown its effectiveness against other species like Mycobacterium tuberculosis,2 non-tuberculous mycobacteria,3 Nocardia sp,4 Actinomadura madurae5, etc., which have broadened the scope of its use. Here, we report a case of actinomycotic mycetoma, non-responsive to the conventional treatment regimen, but showing complete improvement with linezolid monotherapy.
A 14-year-old Indian girl presented with an erythematous indurated plaque over the dorsal aspect of the left foot since 5 years. There was no preceding history of trauma and she did not have any systemic symptom. The plaque was 10 cm x 8.5 cm in size, extending from the ankle up to the dorsal surface of the toes and on the plantar aspect, up to the instep. There were multiple tiny sinuses over the surface of the plaque, along with proliferating granulation tissue [Figure 1]. Grains were not visible on examination. She responded poorly to short courses of oral antibiotics like amoxicillin and azithromycin as well as azole antifungals previously, and the lesion continued to grow in size. A clinical diagnosis of mycetoma was considered. Potassium hydroxide and gram stain smear prepared from the pus did not reveal any organism. Histopathology from the sinus showed grains with a dense mixed inflammatory infiltrate and eosinophilic material deposited around it. On higher magnification, grains were observed to have a variegated pattern with dark basophilic periphery and pale, less dense center, surrounded by eosinophilic material (Splendore Hoeppli phenomenon), characteristic of actinomycotic grain [Figure 2]. The culture from pus and skin biopsy did not grow any organism. Pan fungal polymerase chain reaction was negative. Magnetic resonance imaging of the foot showed heterogeneously enhanced mass on the dorsolateral aspect of the feet with no bone destruction. She was started on a regimen of injection amikacin 15 mg/kg IV daily and tab cotrimoxazole DS 2 tab twice daily. We chose amikacin in place of gentamycin in view of the better side effect profile and preferable once-daily dosing.6 After 1 month of the above regimen; the lesion did not show any significant improvement. According to the regimen in maintenance phase, injection amikacin was stopped and doxycycline 100 mg twice daily was added to cotrimoxazole. In the next 2 months, the lesion became more inflammatory and further progressed in size [Figure 3].
Cotrimoxazole and doxycycline were stopped in view of the lack of response and the patient was started on tablet linezolid 600 mg twice daily. The lesion started to respond within 2 weeks and a complete resolution was seen after 2 months of this therapy [Figure 4]. Complete blood count and liver function tests monitored at monthly intervals were found to be normal. The treatment was continued until 3 months following complete resolution.

- Erythematous indurated plaque with multiple sinuses and granulation tissue over the dorsum of left foot
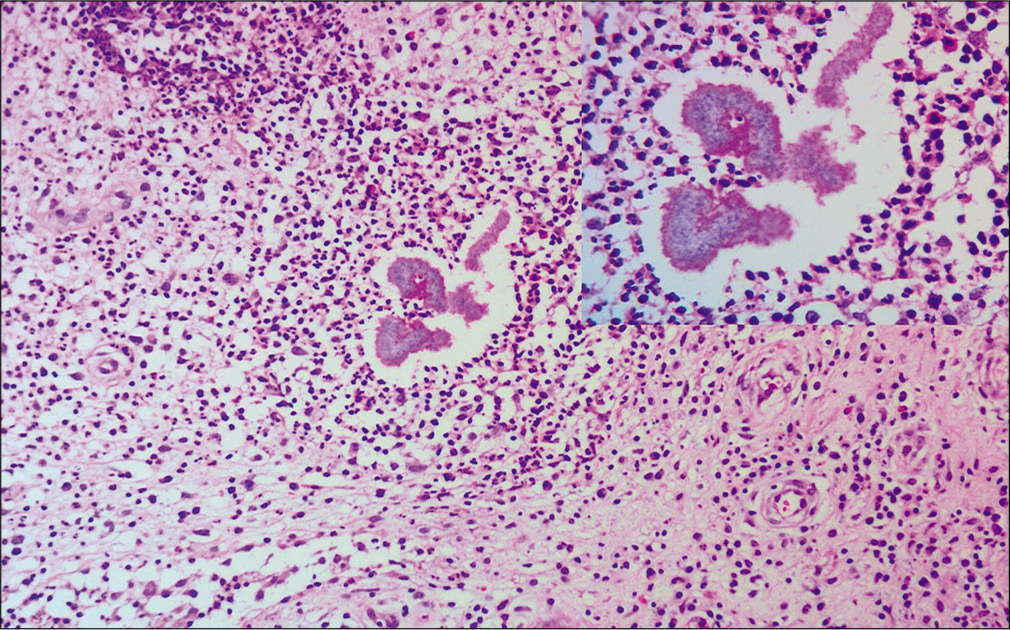
- Dense infiltrate of neutrophils, lymphocytes, histocytes with purple colored actinomycotic grain with eosinophilic material around it (H and E, ×200). Grain was composed of thin filaments (inset: H and E, ×400)

- Increase in the size of the lesion after receiving three months of treatment in the initial regimen

- Complete resolution of the plaque with two months of treatment with linezolid
Mycetoma usually presents with swelling, induration and discharging sinuses over the extremities. Actinomycotic mycetoma is caused by filamentous bacteria like Nocardia brasiliensis, Actinomadura madurae, Actinomadura pelletieri, Streptomyces somaliensis, etc., while eumycotic mycetoma is caused by fungi like Madurella mycetomatis, Trematosphaeria grisea, Falciformispora senegalensis, Falciformispora tompkinsii, etc., Clinical features of these two subtypes are overlapping; thus, histopathological characteristics of grains are the mainstay of diagnosis in most of the cases.7 Special stains like Gram stain, Ziehl– Neelsen staining and potassium hydroxide mount of the grains as well as bacterial and fungal cultures also aid in diagnosis. Various injectable and oral antibiotics have been found to be useful in the management of actinomycotic mycetoma. Culture is negative in majority of the cases, so information regarding antibiotic sensitivity is usually not available and the treatment is given empirically.8 Welsh regimen (consisting of co-trimoxazole with amikacin for 3 weeks, followed by only co-trimoxazole for 2 weeks (constituting 1 pulse) for one to four such cycles9 and modified Ramam’s two-step regimen (“intensive phase” of co-trimoxazole and gentamicin for 4 weeks followed by a “maintenance phase” of co-trimoxazole and doxycycline)10,11 are the commonly used therapeutic regimens. Other modifications of the original Welsh regimen include adding rifampicin, dapsone, doxycycline and streptomycin in different combinations, or increasing the number of cycles, particularly in cases of bony involvement.8 In highly refractory cases, agents such as netilmicin can replace amikacin or an alternative treatment regimen like imipenem alone or with amikacin or amoxicillin–clavulanic acid have been used. Most have shown a cure rate of almost 90% with a treatment non-responsiveness in around 10% of cases.8 Therefore, it is important to have alternative drugs in the management of actinomycetoma. Linezolid has been found to have significant in vitro activity against Actinomadurae spp. and Nocardia spp.4,5 Considering these two species being the commonest causative agents of actinomycotic mycetoma, we considered linezolid as a treatment option, more so, in the setting of a lack of response to the conventional treatment regimen. Till date, though linezolid has been used successfully in the treatment of disseminated systemic Nocardia spp infections in a few occasions, we could not find any clinical study that has used it in the management of actinomycotic mycetoma.12 Considering the good response in our case, linezolid maybe considered as an alternative agent in the treatment of actinomycotic mycetoma.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Linezolid: A promising option in the treatment of Gram positives. J Antimicrob Chemother. 2017;72:354-64.
- [CrossRef] [PubMed] [Google Scholar]
- Linezolid in the treatment of MDR TB: A retrospective clinical study. Int J Tuberc Lung Dis. 2012;16:358-63.
- [CrossRef] [PubMed] [Google Scholar]
- Activities of Linezolid against nontuberculous mycobacteria. New Microbiol. 2007;30:411-4.
- [Google Scholar]
- In vitro activities of linezolid against multiple Nocardia species. Antimicrob Agents Chemother. 2001;45:1295-7.
- [CrossRef] [PubMed] [Google Scholar]
- In vitro activities of new quinolones and oxazolidinones against Actinomadura madurae. Antimicrob Agents Chemother. 2004;48:1037-9.
- [CrossRef] [PubMed] [Google Scholar]
- A prospective comparative study of gentamicin and amikacin induced nephrotoxicity in patients with normal baseline renal function. Fundam Clin Pharmacol. 2009;23:515-20.
- [CrossRef] [PubMed] [Google Scholar]
- Mycetoma: A unique neglected tropical disease. Lancet Infect Dis. 2016;16:100-12.
- [CrossRef] [Google Scholar]
- Drug therapy for Mycetoma. Cochrane Database Syst Rev. 2018;2018:CD013082.
- [CrossRef] [Google Scholar]
- Actinomycetoma and advances in its treatment. Clin Dermatol. 2012;30:372-81.
- [CrossRef] [PubMed] [Google Scholar]
- A two step schedule for the treatment of actinomycotic mycetomas. Acta Derm Venereol. 2000;80:378-80.
- [CrossRef] [PubMed] [Google Scholar]
- A modified two step treatment for actinomycetoma. Indian J Dermatol Venereol Leprol. 2007;73:235-9.
- [CrossRef] [PubMed] [Google Scholar]
- Linezolid for the treatment of Nocardia spp. infections. Ann Pharmacother. 2007;41:1694-9.
- [CrossRef] [PubMed] [Google Scholar]




