Translate this page into:
Lupus vulgaris in a child: A complication of ear piercing
2 College of Medicine and JNM Hospital, Kalyani, West Bengal, India
3 Medical College and Hospital, Kolkata, West Bengal, India
Correspondence Address:
Piyush Kumar
Department of Dermatology, Katihar Medical College and Hospital, Karim Bagh, Katihar - 854 105, Bihar
India
| How to cite this article: Kumar P, Mondal A, Lal NR, Gharami RC. Lupus vulgaris in a child: A complication of ear piercing. Indian J Dermatol Venereol Leprol 2014;80:97 |
Sir,
Childhood cutaneous tuberculosis may constitute 18.7-53.9% of all cutaneous tuberculosis cases. Majority of such cases are seen in children aged 10-14 years and most common clinical type of cutaneous tuberculosis is scrofuloderma, followed by lupus vulgaris. Lupus vulgaris in children is mostly seen on trauma prone parts, usually on legs, knees, thighs, buttocks and feet. [1] However, other sites too may be affected, depending upon the site of inoculation of infective agent. For example, lupus vulgaris at Bacillus Calmette- Guιrin (BCG) vaccination site is well-known. [2] We report a case of the young girl presenting with lupus vulgaris of both ear following ear piercing.
A 9-year-old girl from a rural area presented with asymptomatic erythematous plaques on both ears and surrounding area for 8 months. The lesion first appeared as small erythematous plaque over the right ear, following ear piercing carried out by a neighborhood barber. The lesions slowly progressed in size to present status. New lesions kept appearing in the vicinity of pre-existing lesion and gradually merged with later. There were no features suggestive of middle/inner ear involvement. On examination, well-defined erythematous scaly papules and plaques were noted on both ears, with the right ear affected more severely. There was the extension of lesion from ear to surrounding areas and few satellite lesions could be appreciated [Figure - 1]. There was no cervical or occipital lymphadenopathy and the rest of the mucocutaneous and systemic examination was unremarkable. Peripheral nerve trunk examination did not reveal any thickened nerve trunk. Slit skin smear from lesion was carried out, but no acid-fast bacilli were found on Ziehl-Neelsen staining. Mantoux test with 5-TU showed an induration, sized 12 mm. The punch biopsy from the plaque showed well-formed tubercular granuloma with langhans type of giant cells [Figure - 2]. Routine blood investigations and chest X-ray did not reveal any abnormality. Considering clinical presentation and histopathological findings, diagnosis of lupus vulgaris was made. She was treated with standard anti-tubercular regimen for new cases (category I) and responded very well to treatment.
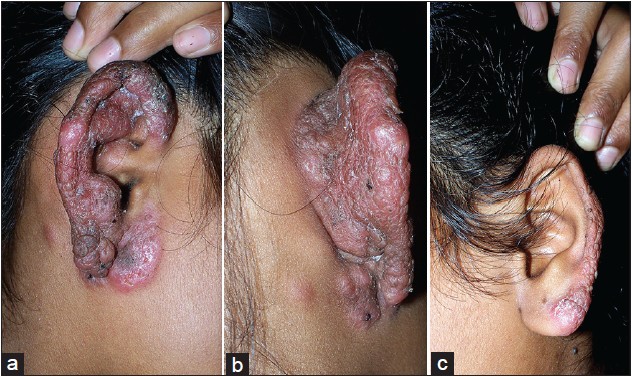 |
| Figure 1: Erythematous scaly papules and plaque on the right ear (a and b) and on the left ear (c) |
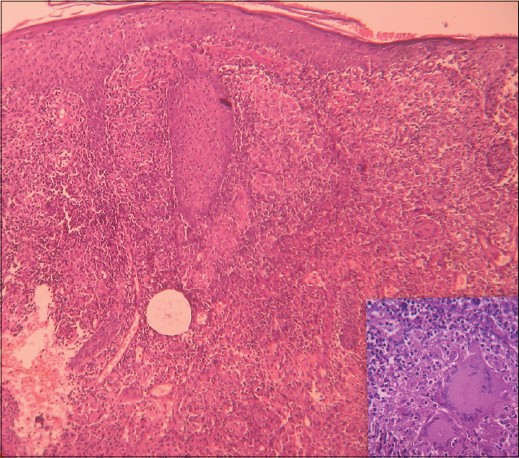 |
| Figure 2: Acanthosis and epidermal atrophy (at places) and wellformed tubercular granuloma in dermis (H and E, ×100). Note langhans type of giant cell (inset, right H and E, ×400) |
Body piercing is the practice of puncturing or cutting a part of the human body, creating an opening, in which jewelry may be worn. Body piercing is almost a routine procedure in Indian females and the commonly pierced sites are ears and nose. However, other sites including lip, tongue, nipple, genitals and navel are pierced too. The practice of body piercing is largely not regulated in India and people usually get it done by neighborhood barber, jeweler or in beauty parlors. Such body piercings usually do not follow aseptic measures or necessary precautions and hence, complications are not uncommon. Most of the complications are universal, irrespective of site pierced; some of them are site specific. The ear lobe is the most frequent site to be pierced and usually free from complications. On the other hand, piercing ears on pinna involves piercing the cartilage that creates a wound that is harder to clean, takes longer to heal and is more likely to become infected than earlobe piercing. Similarly, infection of the lip piercing may cause speech, chewing or swallowing problems or swelling that can block the throat. [3],[4]
The complications common to all sites include bacterial infections (often by common pathogens such as Streptococcus pyogenes and Staphylococcus aureus. tuberculosis and atypical mycobacterial infection, leprosy and syphilis which are uncommon), viral infections (warts, molluscum contagiosum, herpes simplex, blood-transmitted diseases such as hepatitis and human immunodeficiency virus) and fungal infections (sporotrichosis, zygomycosis, even systemic mycoses). The infections may even be limb/life threatening like gangrene, endocarditis or sepsis. Non-infective complications such as hypertrophic scar, keloid and pyogenic granuloma too are common. [3],[4] Some dermatological conditions such as psoriasis and vitiligo may develop at trauma site (Koebner phenomenon). Apart from these complications, there is always a risk of unanticipated physical injuries such as damage to underlying blood vessels or nerves, when piercing is carried out by untrained persons. [5] Jewelry worn after piercing too is associated with complications and may cause allergic contact dermatitis in susceptible persons, most frequently due to its nickel content. Heavier jewelry, due to constant stretching, often causes elongated piercing tracts or even torn earlobes, which may require surgical repair. To avoid complications, body piercing should be practiced in strict aseptic conditions using specialized instruments such as piercing needle. Furthermore, the jewelry should be hypoallergenic. Gold should be avoided in initial piercings as it is mixed with other metals. Surgical stainless steel, platinum and palladium are less likely to cause an allergic reaction. [4]
| 1. |
Singal A, Sonthalia S. Cutaneous tuberculosis in children: The Indian perspective. Indian J Dermatol Venereol Leprol 2010;76:494-503.
[Google Scholar]
|
| 2. |
Thakur BK, Verma S. BCG-induced lupus vulgaris complicated by squamous cell carcinoma in a 7-year-old child. Int J Dermatol 2011;50:542-5.
[Google Scholar]
|
| 3. |
Stirn A. Body piercing: Medical consequences and psychological motivations. Lancet 2003;361:1205-15.
[Google Scholar]
|
| 4. |
Holbrook J, Minocha J, Laumann A. Body piercing: Complications and prevention of health risks. Am J Clin Dermatol 2012;13:1-17.
[Google Scholar]
|
| 5. |
Park MH, Mehran A. Intestinal injury secondary to an umbilical piercing. JSLS 2012;16:485-7.
[Google Scholar]
|
Fulltext Views
4,119
PDF downloads
3,023





![[Figure - 1]](#fig_ijdvl_2014_80_1_97_125526_u1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2014_80_1_97_125526_u2.jpg){kind=link}