Translate this page into:
Madelung's disease: A benign symmetric lipomatosis
Correspondence Address:
Gaurav Dash
Deulasahi in front of Monalisa Palace, Tulsipur, Cuttack, Odisha - 753 008
India
| How to cite this article: Mohanty P, Vivekanandh K, Dash G, Mohapatra L. Madelung's disease: A benign symmetric lipomatosis. Indian J Dermatol Venereol Leprol 2018;84:190-191 |
Sir,
Madelung's disease, also known as benign symmetrical lipomatosis, Launois–Bensaude syndrome, Brodie syndrome, Buschke disease and multiple symmetrical lipomatosis, is a rare acquired disorder of fat metabolism. It is characterized by multiple lipomas which are symmetrically distributed; mainly around the upper trunk, neck and shoulders.[1] Males of the age group, 30–60 years are the most commonly affected. It is associated with chronic alcohol use and has varied manifestations such as dyspnea, dysphagia, polyneuropathy and muscle weakness. It usually causes cosmetic concern.[2] Around 200 and odd cases have been reported worldwide [3] and yet there are very few case reports in the Indian literature.
A 38-year-old male presented to the dermatology out-patient department of S.C.B. Medical College and Hospital, Cuttack, Odisha, with complaints of painless, slowly progressive, disfiguring swellings over his shoulders, arms and upper trunk since childhood. There was no history of dyspnoea or dysphagia, drug use or other medical conditions. He was a light drinker, taking four units of alcohol per week for the past 10 years. The patient was operated twice before, but the lesions used to recur in a few years. On examination, there were diffuse, soft to firm, skin colored subcutaneous masses over his shoulders, arms and upper trunk [Figure - 1]. The lesions were non-tender and freely mobile. No lymphadenopathy was present. Other general, systemic and dermatological examination findings were unremarkable.
 |
| Figure 1: Symmetric diffuse lipomatous swellings over the shoulders, arms and upper trunk |
Routine laboratory investigations, lipid profile, liver function tests and endocrinological investigations were within normal limits. Excisional biopsy was done. Histopathological examination showed clusters of mature adipocytes. Computed tomography (CT) scan showed diffuse fat attenuation in the upper thoracic, bilateral shoulder and arm regions, with no mediastinal involvement [Figure - 2]. Based on the above findings, a final diagnosis of Madelung's disease was made.
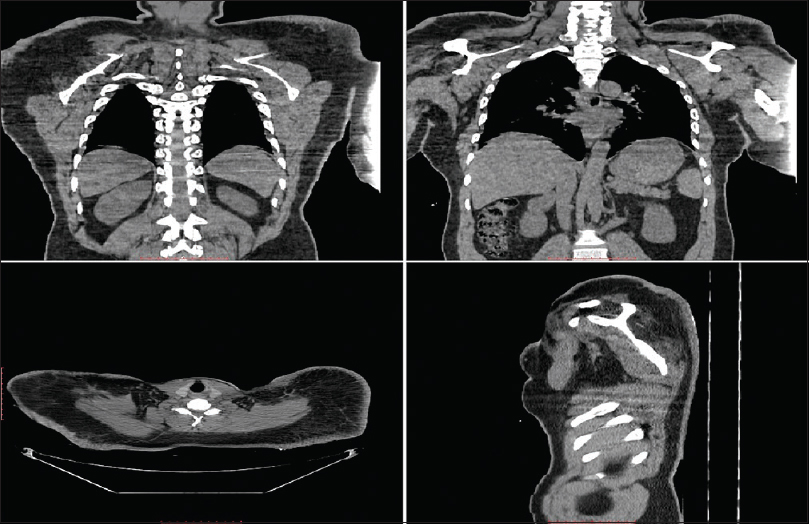 |
| Figure 2: Diffuse fat attenuation in the upper thoracic, bilateral shoulder and arm regions |
As the patient was asymptomatic and not much concerned about cosmesis, we did not prefer surgery. He was managed conservatively. He was counseled about the nature of the disease, was advised to avoid alcohol intake and report to the doctor in the event of developing any new symptoms. The patient stopped consuming alcohol and there was no further progression of the lesions during the 6 months follow-up period.
Madelung's disease, first reported in 1846 by Brodie, was called 'fat neck' (Fetthals) by Madelung.[4] In 1888, Otto Madelung reported the first series of 33 patients with lipomas associated with alcoholism, and in the next year, Launois and Bensaude presented a total of 65 patients with similar features. It is characterized by symmetric deposits of non-encapsulated adipose tissue in the upper trunk, neck, shoulders and arms. Massive deposition of fat becomes cosmetically deforming in the parotid region (“hamster cheeks”), cervical region (“horse collar”) and posterior neck (“buffalo humps”), giving the patient a “pseudo-athletic appearance.”[5] It predominantly affects middle-aged men of Mediterranean origin.
Most of the patients have history of alcoholism, but it is also reported in non-alcoholics and females. The other associated conditions include diabetes mellitus, hyperlipoproteinemia, hypothyroidism, gout and systemic mitochondrial diseases. Some patients also present with peripheral neuropathy, autonomic nervous system manifestations and symptoms due to compression of the airway, esophagus, carotids or venacava.[4]
The cause of Madelung's disease is unknown; many hypotheses have been proposed. The pathogenesis of this disease is suspected to be a defect in adrenergic stimulated lipolysis, resulting in massive accumulation of lipomatous tissue. Another theory of accumulation of embryological brown fat has also been proposed.[6] Recently, Madelung's disease has been recognized in two clinical phenotypes. Type 1 affects men primarily and is characterized by fatty tissue accumulation around the neck, nape of the neck, upper back, shoulders and upper arms. Type 2 affects both men and women, producing an exaggerated female fat tissue distribution in the upper back, deltoid region, upper arms, hips and the upper thigh regions.[7]
The workup for this disease includes detailed clinical examination, sonography, computerized tomography and fine-needle aspiration cytology. The important differential diagnoses include liposarcoma, multiple familial lipomatosis, Dercum's disease, neurofibroma, drug-induced lipomatosis (steroidal and antiretroviral drugs), angiolipoma and hibernoma.[4]
Abstinence from alcohol prevents progression of the disease. Diet modification has no role in the management. Medical therapy with thyroid extracts, vitamins and beta 2-agonists such as salbutamol (for lipolysis stimulation) have been tried but not been very effective.[2] Surgical treatment includes lipectomy and liposuction. Surgery is reserved for patients who have severe aesthetic deformities or are symptomatic (dyspnea, dysphagia), as malignant transformation is extremely rare and recurrence is common because of the inability to completely excise the fat tissue.[7]
Our patient had none of the associated diseases except for alcoholism. We treated the patient conservatively because he had no other complaints related to the excess fat tissue. Increasing awareness of the presence of this rare disease in our medical community could prevent misdiagnosis and misleading management. Typical morphology and distribution of the lesions should make the diagnosis simple. We could find only two such cases previously reported from India.[4]
Acknowledgement
Dr. Archana Jayakumar, M.D. (Radiodiagnosis).
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patient has given the consent for the images and other clinical information to be reported in the journal. The patient understands that name and initials will not be published and due efforts will be made to conceal identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
| 1. |
Ardeleanu V, Chicos S, Georgescu C, Tutunaru D. Multiple benign symmetric lipomatosis – A differential diagnosis of obesity. Chirurgia (Bucur) 2013;108:580-3.
[Google Scholar]
|
| 2. |
Bulum T, Duvnjak L, Car N, Metelko Z. Madelung's disease: Case report and review of the literature. Diabetol Croat 2007;36:25-30.
[Google Scholar]
|
| 3. |
Fonseca VA, Alves C, Marques H, Camacho E, Saraiva AP. Madelung's disease as a rare cause of obstructive sleep apnea. J Bras Pneumol 2009;35:1053-6.
[Google Scholar]
|
| 4. |
Medappil N, Vasu TA. Madelung's disease: A spot diagnosis. Indian J Plast Surg 2010;43:227-8.
[Google Scholar]
|
| 5. |
Josephson GD, Sclafani AP, Stern J. Benign symmetric lipomatosis (Madelung's disease). Otolaryngol Head Neck Surg 1996;115:170-1.
[Google Scholar]
|
| 6. |
Suresh Chandran CJ, Godge YR, Oak PJ, Ravat SH. Madelung's disease with myopathy. Ann Indian Acad Neurol 2009;12:131-2.
[Google Scholar]
|
| 7. |
Hirose A, Okada Y, Morita E, Tanaka Y. Benign symmetric lipomatosis associated with alcoholism. Intern Med 2006;45:1001-5.
[Google Scholar]
|
Fulltext Views
4,633
PDF downloads
2,293





![[Figure - 1]](#fig_ijdvl_2018_84_2_190_224872_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2018_84_2_190_224872_f2.jpg){kind=link}