
Translate this page into:
Modified acne scar revision - Punch excision, punch-in-subcision with shoulder dermabrasion followed by dermal grafting
Corresponding author: Dr. Sushil S. Savant Jr, Department of Dermatology, The Humanitarian Clinic: Skin, Hair and Laser Centre, Andheri West, Mumbai, Maharashtra, India. sushilsavant786@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Savant Jr SS. Modified acne scar revision - Punch excision, punch-in-subcision with shoulder dermabrasion followed by dermal grafting. Indian J Dermatol Venereol Leprol. 2025;91:139-41. doi: 10.25259/IJDVL_914_2023
Problem
Both crateriform and ice pick varieties cannot be revised satisfactorily by dermabrasion or laser ablation alone as they cannot reach the requisite depth for effective management.1,2 Our proposed novel technique combines punch excision followed by punch-in-subcision, shouldering dermabrasion and dermal grafting for modifying acne scar revision.
Solution
Surgical preparation was marked [Figure 1a]. Lignocaine (1%) was administered as local infiltration intradermally and subcutaneously. The recipient site involved scar removal using biopsy punches of the same size as scar tissue (1.0–2.5 mm) deep up to the subcutaneous fat, lifted up, cut and discarded [Figure 1b]. Already punched out chambers were dilated with a 0.5 mm larger punch guard. The scar was pierced, punched-out with an injection needle 21G to 16G (bevel pointing up)/18G-1.5 inch Nokor needle (blade pointing up)/myringotomy knife and advanced angularly (≈45°–30° to skin surface) to a level below the scar. The needle/blade was then tilted horizontally (parallel to the skin surface) just below the deep dermal or dermal subcutaneous junction and moved back and forth through the scar until loss of resistance was felt. To and fro subcision via punch-in targets surrounding scarred tissue thus achieving a synergistic approach to both surrounding scars and specific punch-excised scars. A snapping sound indicates breaking of bands. The forward and backward piston-like movement was used to advance the needle through fibrous bands to release them. Overlying tissue was mobilised over the penetrated needle (punch-in-subcision) [Figure 1c]. Individual punched-out scar surfaces were moderately stretched. Using a pear-shaped diamond fraised end-piece and pencil-like vertical grip of the hand machine, the handpiece is gently rotated clockwise in small circles to lightly abrade the scarbase and firmly abraded edges. Similarly, the marked scars were individually smoothened out. Dermabrasion mechanically smoothens edges and diminishes crateriform appearance, particularly effective in rolling scars (shoulder dermabrasion) [Figure 1d]. Donor site preparation involved surgical preparation of the post-auricular area and dermabraded (manual/electrical/combination) overlying skin surface till complete removal of epidermis and occurrence of pinpoint bleeding [Figure 1e]. Circular punch grafts (0.5 mm larger in diameter than excised scar) descended up to subcutaneous fat. It was gently lifted, the base was cut and then stored after removing fat that grafts contained only dermal tissue (dermal graft) [Figure 2a]. Dermal grafts were stored in sterile petri dishes containing moist (normal saline) gauze pieces. The donor site was either sutured with 3-0 proline or allowed to heal by secondary intention. It was dressed in antibiotic cream or framycetin/bactigras tulle and gauze pieces. Dermal grafts were individually transferred to suitable chambers, trimmed for a snug fit if required and haemostasis was achieved [Figure 2b]. Postoperative medications (antibiotics and anti-inflammatory drugs) were given for 8–10 days. Follow-up dressing included: (a) Recipient site: suture was removed after 7–10 days as needed and (b) Donor site: opened after 7 days, the suture was removed if sutured [Figure 2c]. Scars improved gradually by secondary intention through re-epithelialisation from wound margins [Figure 2d] and remarkable cosmetic improvement was noted after 1 month [Figure 2e and video].
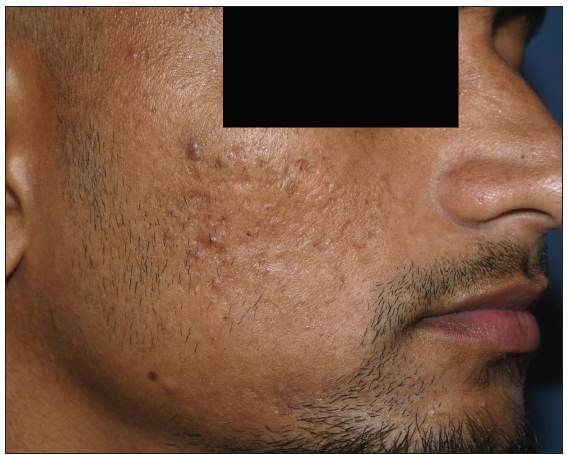
- Post acne scars (rolling type) at baseline.

- Intra-operative: Punch excision of individual recipient area scars.

- Punch-in-subcision to target underlying fibrosis and upliftment of recipient area.

- Shoulder dermabrasion to abrade the base and edges.

- De-epidermisation of the donor site (retroauricular area).

- Harvesting dermal grafts from donor site (retroauricular area).

- Transfer of dermal graft to recipient area over an individual scar.
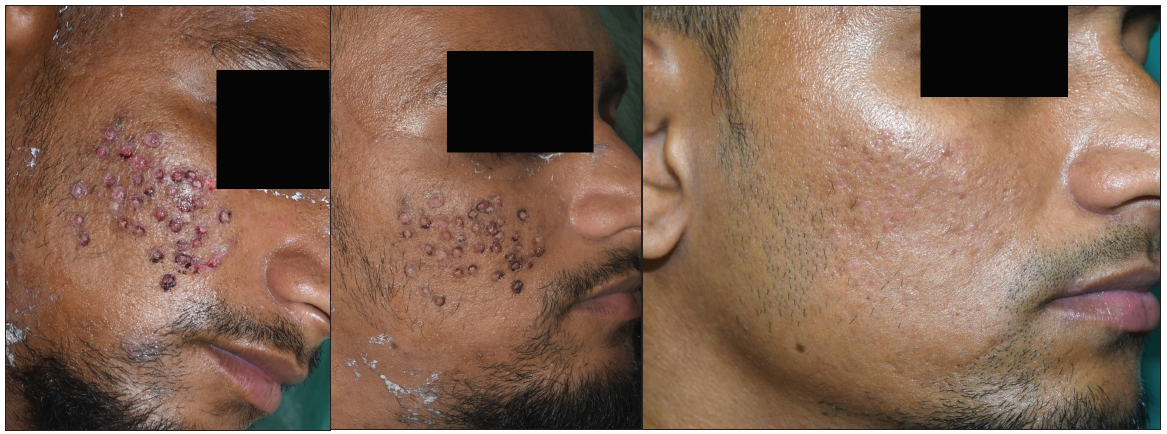
- (c) Recipient area after 7 days of treatment, (d) after 14 days and (e) after 1 month of treatment.
Declaration of patient consent
The author certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The author confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
References
- Pitted facial scar revision. In: Textbook of dermatosurgery & cosmetology: Principles and practice (3rd ed). Mumbai, India: Bhavani Publishing House; 2018. p. :334-5.
- [Google Scholar]
- Dermabrasion. In: Textbook of dermatosurgery & cosmetology: Principles and practice (3rd ed). Mumbai, India: Bhavani Publishing House; 2018. p. :346-67.
- [Google Scholar]




