Translate this page into:
Multinucleated giant cells in angiolymphoid hyperplasia with eosinophilia
2 Department of Dermatology, Vardhman Mahavir Medical College and Safdarjung Hospital, New Delhi, India
Correspondence Address:
Avninder Singh
National Institute of Pathology (ICMR), Safdarjung Hospital Campus, New Delhi - 110 029
India
| How to cite this article: Kaur M, Dalal V, Ramesh V, Singh A. Multinucleated giant cells in angiolymphoid hyperplasia with eosinophilia. Indian J Dermatol Venereol Leprol 2016;82:567-569 |
Sir,
A 45-year-old woman presented with multiple asymptomatic, erythematous, firm, smooth nodules on the right side of scalp for 8 years [Figure - 1]. The differential diagnoses of cylindroma, angiolymphoid hyperplasia with eosinophilia and angiosarcoma were considered and a biopsy taken from one of the lesions. Histopathological examination showed an atrophic epidermis with proliferation of blood vessels in the dermis that were lined by plump endothelial cells surrounded by lympho-histiocytes and eosinophils. In addition, a few multinucleated giant cells were seen interspersed among the inflammatory cells [Figure - 2]. No atypia or mitosis was seen. No anastomosing vascular channels were found. With these features, a diagnosis of angiolymphoid hyperplasia with eosinophilia was made.
 |
| Figure 1: Erythematous nodular lesions on the scalp |
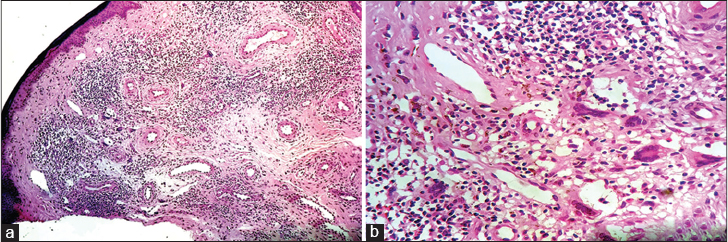 |
| Figure 2: (a) Dermis with proliferating blood vessels surrounded by a dense inflammatory infiltrate with giant cells (H and E, ×100). (b) Giant cells under high power (H and E, ×400) |
Immunohistochemical staining with the markers CD34 and CD68 was performed to ascertain the origin (endothelial/histiocytic) of the giant cells in the infiltrate. These cells expressed CD68 suggesting a histiocytic lineage [Figure - 3], while they were negative for CD34.
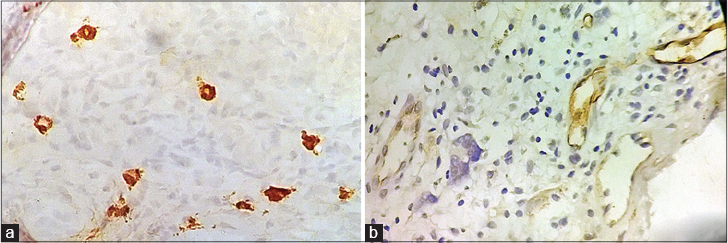 |
| Figure 3: (a) Immunohistochemistry showing CD68 positivity in giant cells (×400). (b) Giant cells negative for CD34 (internal control - blood vessels) (×400) |
Angiolymphoid hyperplasia with eosinophilia, also known as epithelioid hemangioma, is a rare benign vascular tumor. The condition was first described in 1969 and the term epithelioid hemangioma was introduced in 1982.[1] The most common clinical presentation is in the form of single or multiple red-brown papules or nodules, ranging in size from a few to several centimetres. Peripheral blood eosinophilia is seen in 20% of patients, possibly due to the increased circulating interleukin-5 levels.[2]
Histopathologically, it is characterized by a proliferation of blood vessels lined by plump histiocytoid endothelial cells which are characteristically “epithelioid” in appearance with a large nucleus and abundant eosinophilic cytoplasm. Prominent cytoplasmic vacuoles are sometimes seen. Surrounding these blood vessels, an inflammatory infiltrate composed of lymphocytes, varying amounts of eosinophils and mast cells is seen. The endothelial and inflammatory cells are typically bland. Either component may dominate, depending on the age of the lesion.[2]
The presence of multinucleated giant cells in angiolymphoid hyperplasia with eosinophilia has rarely been described. We were able to find only two previous cases, one showing giant cells intermixed with the usual inflammatory infiltrate around the blood vessels and the other with giant cells occurring in association with a diffuse granulomatous reaction in a 34-year-old pregnant woman.[3],[4] Sakamoto et al. have proposed that these giant cells are histogenetically of two types: endothelial type with expression of Factor VIII and Ulex europaeus agglutinin-1 and the second type with of fibrohistiocytic origin.[3] Ultrastructurally, the former show organelles with Weibel–Palade bodies, similar to those seen in endothelial proliferations. The latter have dilated rough endoplasmic reticulum, discontinuous plaques on plasma membrane and pinocytic vesicles indicating differentiation toward a fibrohistiocytic lineage. In our case, the giant cells were positive for the histiocytic marker, CD68 and negative for the endothelial marker, CD34.
The main differential diagnoses include Kimura disease, angiosarcoma and multinucleated cell angiohistiocytoma. Angiolymphoid hyperplasia with eosinophilia and Kimura disease were considered to be the same entity in the past. However, recent studies have shown them to be distinct clinical and histopathologic entities. Kimura disease typically presents as one or more large subcutaneous nodular masses in the periauricular or submandibular region with peripheral eosinophilia, typically in a young Asian male. Histopathologically, florid lymphoid follicles with germinal center formation, eosinophilic infiltrates, eosinophilic microabscesses and eosinophilic folliculolysis are seen. However, the typical epithelioid appearance of endothelial cells, as seen in angiolymphoid hyperplasia with eosinophilia, is lacking.[2],[5]
Angiosarcoma can be distinguished by its characteristic anastomosing vascular channels and atypical appearance of the lining endothelial cells.[2] The presence of multinucleated giant cells in association with dermal vascular proliferation is also seen in multinucleate cell angiohistiocytoma. It presents as multiple, dome-shaped, pink or red papules, mostly on the extremities with occasional involvement of the face. It can be differentiated from angiolymphoid hyperplasia with eosinophilia by the sparseness of the infiltrate which is comprised mainly of lymphocytes and plasma cells, with an absence of eosinophils.[6]
Angiolymphoid hyperplasia with eosinophilia follows a benign clinical course with no metastases reported so far. Surgical excision is the treatment of choice and when completely excised, it rarely recurs.[2]
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
| 1. |
Weiss SW, Enzinger FM. Epithelioid hemangioendothelioma: A vascular tumor often mistaken for a carcinoma. Cancer 1982;50:970-81.
[Google Scholar]
|
| 2. |
Guo R, Gavino AC. Angiolymphoid hyperplasia with eosinophilia. Arch Pathol Lab Med 2015;139:683-6.
[Google Scholar]
|
| 3. |
Sakamoto F, Hashimoto T, Takenouchi T, Ito M, Nitto H. Angiolymphoid hyperplasia with eosinophilia presenting multinucleated cells in histology: An ultrastructural study. J Cutan Pathol 1998;25:322-6.
[Google Scholar]
|
| 4. |
Macarenco RS, do Canto AL, Gonzalez S. Angiolymphoid hyperplasia with eosinophilia showing prominent granulomatous and fibrotic reaction: A morphological and immunohistochemical study. Am J Dermatopathol 2006;28:514-7.
[Google Scholar]
|
| 5. |
Briggs PL. Kimura disease is not angiolymphoid hyperplasia with eosinophilia: Clinical and pathological correlation with literature review and definition of diagnostic criteria. An Bras Dermatol 2006;2: 167-73.
[Google Scholar]
|
| 6. |
Jaconelli L, Kanitakis J, Ktiouet S, Faure M, Claudy A. Multinucleate cell angiohistiocytoma: Report of three new cases and literature review. Dermatol Online J 2009;15:4.
[Google Scholar]
|
Fulltext Views
4,476
PDF downloads
1,773





![[Figure - 1]](#fig_ijdvl_2016_82_5_567_182977_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2016_82_5_567_182977_f2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2016_82_5_567_182977_f3.jpg){kind=link}