Translate this page into:
Multiple congenital vascular lesions in a child
Correspondence Address:
Filipa Diamantino
Department of Dermatology, Hospital of Capuchos, Hospital Center of Central Lisbon, 1169-050 Lisboa
Portugal
| How to cite this article: Diamantino F, V, Alexandre J, Bapstista J. Multiple congenital vascular lesions in a child. Indian J Dermatol Venereol Leprol 2011;77:627 |
Sir,
A 6-year-old girl was referred to our department for evaluation of vascular lesions on her left forearm and chest that had been noticed at birth. They were asymptomatic and gradually increased with her age. Otherwise the child was healthy and had no history of gastrointestinal bleeding or hematuria. The family history was negative for similar lesions.
Physical examination of the left forearm showed an indurated and bluish plaque with overlying coalescent blue and violaceous macules and papules [Figure - 1]a. On the left supramammary region she had two purplish patches with telangiectatic vessels on their surface [Figure - 1]b. The lesions were partially compressible and nontender to palpation and bruits were absent on auscultation.
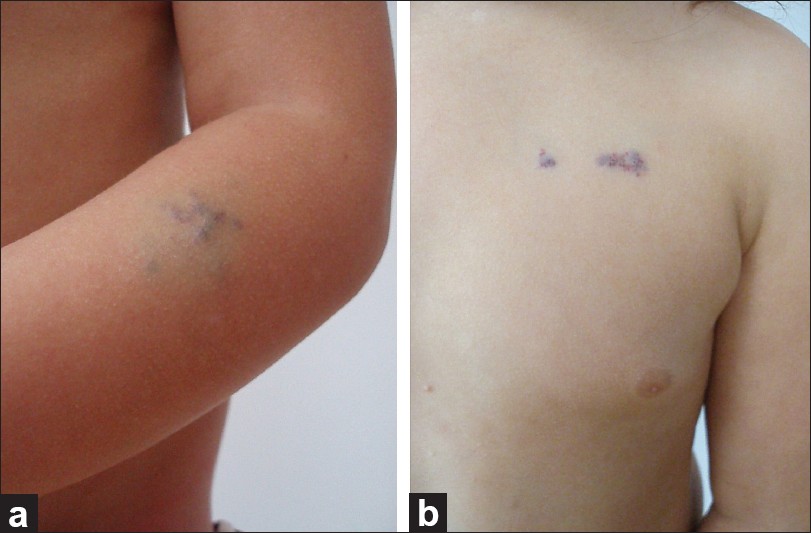 |
| Figure 1: (a) Indurated plaque with overlying coalescent blue and violaceous macules and papules on the left forearm; -(b) purplish patches with telangiectatic vessels on the left supramammary region |
Laboratory values, including complete blood cell and platelet counts, were normal. The abdominal echography failed to detect any internal vascular lesion.
Histopathologic examination revealed a normal epidermis and numerous dilated vascular spaces within the dermis. The thin endothelial cells of the vascular wall were surrounded by several layers of cuboidal cells with broad eosinophilic cytoplasm and round, uniform nuclei [Figure - 2]a. The findings were consistent with the diagnosis of glomuvenous malformation (GVM), which was further supported by strong immunoreactivity of tumor cells with α-muscle actin [Figure - 2]b. The patient and her parents refused treatment and she is currently under observation.
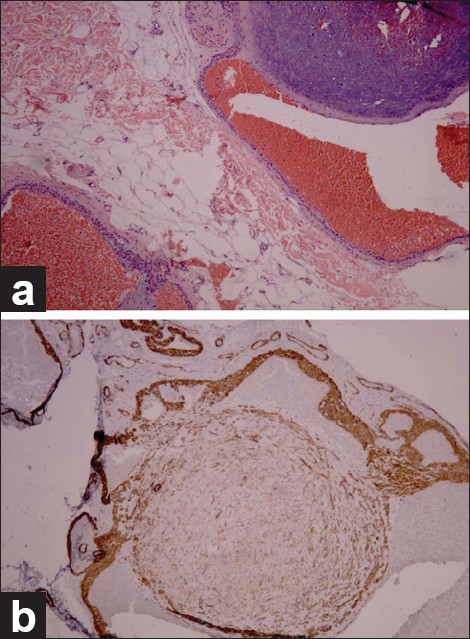 |
| Figure 2: (a) Skin biopsy exhibits a normal epidermis and enlarged vascular spaces lined by a thin layer of endothelial cells, which are surrounded by one or two rows of round, monomorphic cells (H and E, ×400), (b) immunohistochemical staining: positive for smooth muscle α -actin (immunohistochemical staining with antibody against smooth muscle cell α -actin, magnification ×100) |
GVMs combine features of both venous malformations and proliferation of glomus cells. [1] Formerly known as glomus tumors or glomangiomas, those lesions have been renamed GVMs to stress the fact that they are not neoplastic. [2]
GVMs are clinically classified as solitary or multiple. The former are the most common type and consist of solitary nodules that occur mostly in young adults, with female preponderance. Those nodules are characteristically shown on the fingers, mainly in the nail bed. Multiple GVMs-less than 10% of all reported cases-having their onset at earlier ages, consist of red to blue, compressible papulonodules, which tend to be less painful. They are mostly found on the trunk and vary in number from a few to hundreds. [2],[3] Multiple GVMs can be subdivided into localized, disseminated, and congenital plaque-type forms. [3] This third and rare variant, in which category we include our case, was first described by Landthaler et al in 1990. [4]
GVMs can be due to a sporadic mutation or inherited in an autosomal-dominant fashion with variable penetrance and expression. Affected individuals and carriers have heterozygous germline mutations in the glomulin gene (GLMN) that cause a premature stop codon and a truncated glomulin protein. [2] According to Happle and Konig, [5] the plaque-type GVM, superimposed on the ordinary phenotype of this autosomal dominant disorder, is classified as a type two segmental manifestation caused by loss of heterozygosity in the embryo.
Histologically, GVMs are nonencapsulated tumors with large, irregular cavities similar to venous malformations, but the vascular spaces are lined by one or two layers of these round or polygonal glomus cells. The glomus cells closely resemble the modified smooth muscle cells of a specialized arteriovenous shunt, called the Sucquet-Hoyer channel or glomus body. Each cell has an eosinophilic cytoplasm and round, central nuclei. As modified smooth muscle cells, they are immunoreactive to actin and vimentin. Multiple GVM are less well circumscribed and less solid-appearing than solitary GVMs. [3],[4]
This specific congenital plaque-type of GVM presents as subtle, flat, pink or bluish plaques present since birth that enlarge proportionately with body growth and become deep, dark, blue plaques. Any part of the body may be affected. Later in life, often during puberty, most patients develop new papules and nodules on distinct areas from those involved at birth. [2],[3],[4]
The treatment of GVM largely depends on the number, extent, and location of the lesions. Treatment options include surgical excision, sclerotherapy, and laser therapy (ablative or pulsed dye). [1],[3]
The patient herein described is an example of the rare, congenital plaque-like GVM. We consider that the histopathologic examination is essential to clarify the diagnosis and that the recognition of the benign nature of this entity and the follow-up of patients is important. Genetic screening for glomulin was not performed as it is not commercially available yet.
| 1. |
Henning JS, Kovich OI, Schaffer JV. Glomovenous malformations. Dermatol Online J 2007;13:17.
[Google Scholar]
|
| 2. |
Chen AY, Eide M, Shwayder T. Glomuvenous malformations in a boy with transposition of the great vessels: a case report and review of literature. Pediatr Dermatol 2009;26:70-4.
[Google Scholar]
|
| 3. |
Mallory SB, Enjolras O, Boon LM, Rogers E, Berk DR, Blei F, et al. Congenital plaque-type glomuvenous malformations presenting in childhood. Arch Dermatol 2006;142:892-6.
[Google Scholar]
|
| 4. |
Landthaler M, Braun-Falco O, Eckert F, Stolz W, Dorn M, Wolff HH. Congenital multiple plaquelike glomus tumors. Arch Dermatol 1990;126:1203-7.
[Google Scholar]
|
| 5. |
Happle R, Konig A. Type 2 segmental manifestation of multiple glomus tumors: A review and reclassification of 5 case reports. Dermatology 1999;98:270-2.
[Google Scholar]
|
Fulltext Views
2,293
PDF downloads
1,869





![[Figure - 1]](#fig_ijdvl_2011_77_5_627_84084_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2011_77_5_627_84084_f2.jpg){kind=link}