Translate this page into:
Multiple giant clear cell acanthomas
2 Department of Pathology, Medical Faculty, Bezmialem Vakif University, Istanbul, Turkey
3 Department of Pathology, Cerrahpasa Medical Faculty, Istanbul University, Istanbul, Turkey
Correspondence Address:
Ozlem Su
Department of Dermatology and Venereology Medical Faculty, Bezmialem Vakif University, Fatih, Istanbul
Turkey
| How to cite this article: Su O, Dizman D, Onsun N, Ozkaya DB, Tosuner Z, Bahali AG, Demirkesen C. Multiple giant clear cell acanthomas. Indian J Dermatol Venereol Leprol 2016;82:218-221 |
Sir,
Clear cell acanthoma, first described by Degos in 1962, [1] was originally thought to be a benign epidermal tumor. However, recent studies suggest that it is a reactive inflammatory dermatosis. Immunohistochemically, it shows a staining pattern similar to inflammatory dermatoses such as psoriasis vulgaris, lichen planus and discoid lupus erythematosus. The etiology remains unknown. [1],[2] The lesion is typically slow-growing, asymptomatic, solitary and located on the legs, although all parts of the body can be affected. It tends to affect people aged 50-70 years and usually consists of a sharply demarcated, dome-shaped nodule or plaque, 5-20 mm in diameter. The most characteristic clinical features are a thin wafer-like scale forming a peripheral collarette, slight moisture and numerous pin-point sized blanchable vascular punctae scattered over the surface.
An 81-year-old woman was seen in the department of dermatovenereology, Bezmialem Vakif University Hospital, Istanbul, Turkey, complaining of itchy papules and nodules on both lower extremities. She reported that these nodules first appeared on the right calf 40 years ago. Twenty years later, satellite papules started appearing around the initial, larger nodule on her right calf. Subsequently, similar lesions were noted on the left leg and both thighs. The lesions had been itching and bleeding over the last few years. Her past medical history was significant for hypertension and hypothyroidism for which she was on levothyroxine and atenolol/chlorthalidone. None of her family members had similar lesions. On physical examination, there was a 40 mm × 30 mm, red, sharply demarcated nodule with satellite papulo-nodules on her right calf. There were scattered, well defined papules and nodules (5-15 mm) with a thin rim of scale on both posterior lower extremities. Three biopsies were performed from lesions from both legs [Figure - 1].
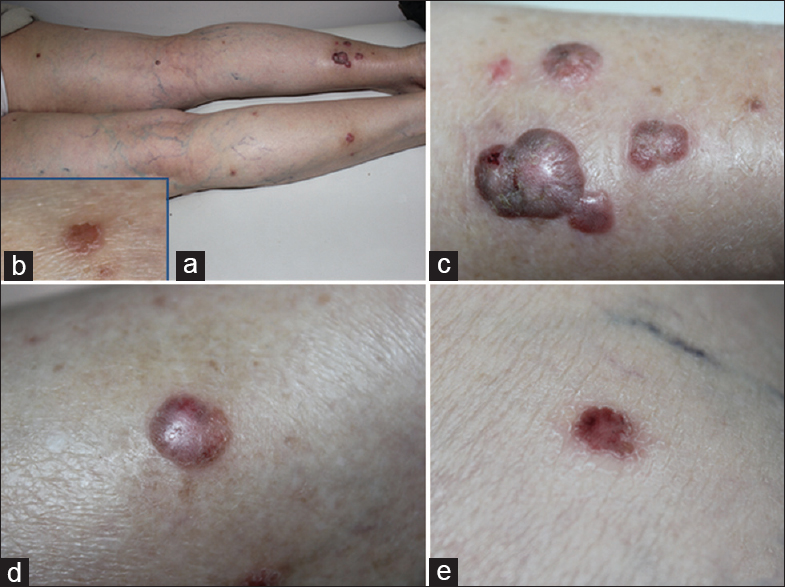 |
| Figure 1: Appearance of the posterior side of lower extremities (a). There was a 40 mm × 30 mm red, sharply demarcated nodule and 10 mm × 20 mm satellite papulonodules around it on her posterior side of right leg (c). There was scattered 5 mm, 10 mm, 15 mm papules and nodules with sharply demarcated margins and a thin collateral rim of scale on her posterior side of both lower extremities (b,d and e) |
On histological examination, there was epidermal acanthosis with the proliferation of clear cells containing intracytoplasmic glycogen. Periodic-acid-Schiff staining was positive. Clear demarcation was seen between the lesion and adjacent normal epidermis. There were neutrophils in the stratum corneum. The blood vessels in the papillary dermis were dilated and increased in number. Based on these findings, a diagnosis of multiple clear cell acanthoma was made [Figure - 2].
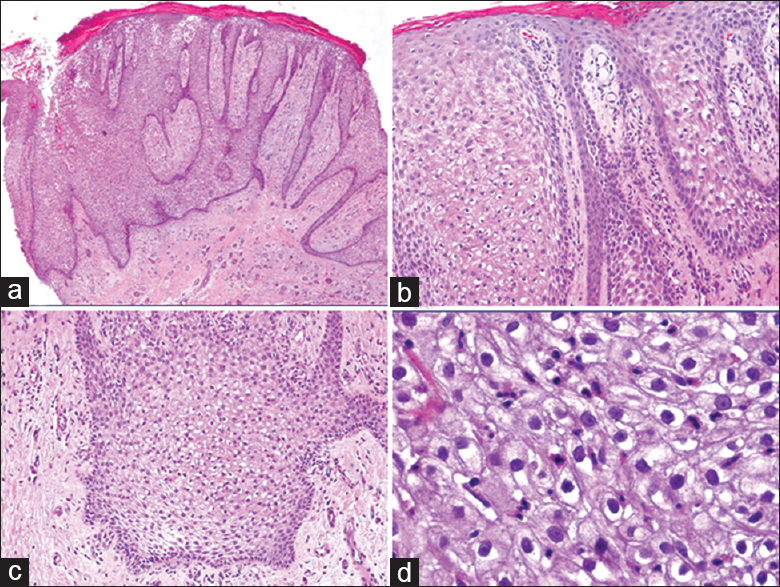 |
| Figure 2: On histological examination epidermal acanthosis, pale appearance of the keratinocytes and intraepidermal neutrophils were seen. In the dermis, there was proliferation of blood vessels and perivascular infiltration of lymphocytes, histiocytes and neutrophils. (a) H and E, ×40 (b) H and E, ×100 (c) H and E, ×100 (d) H and E, ×200 |
The first case of multiple clear cell acanthoma was described in 1964 by Delacretaz et al.[3] Several variants of the condition including giant, polypoid, pigmented and eruptive patterns have been described. The eruptive form is characterized by more than 30 papules which arise within a month. Multiple and giant forms are rare; we were able to find 38 cases of multiple and 9 giant clear cell acanthoma in the literature. Two out of the nine cases of giant clear cell acanthomas had multiple lesions. Langtry et al. reported a case with multiple giant (40 mm) lesions and a lesion 10 mm × 12 mm in size on the left buttock of an 87-year-old woman. [4] Kim et al. reported a 14-year-old girl with a 2-month history of two erythematous nodules measuring 20 mm × 32 mm and 40 mm × 55 mm on the perianal area. [5]
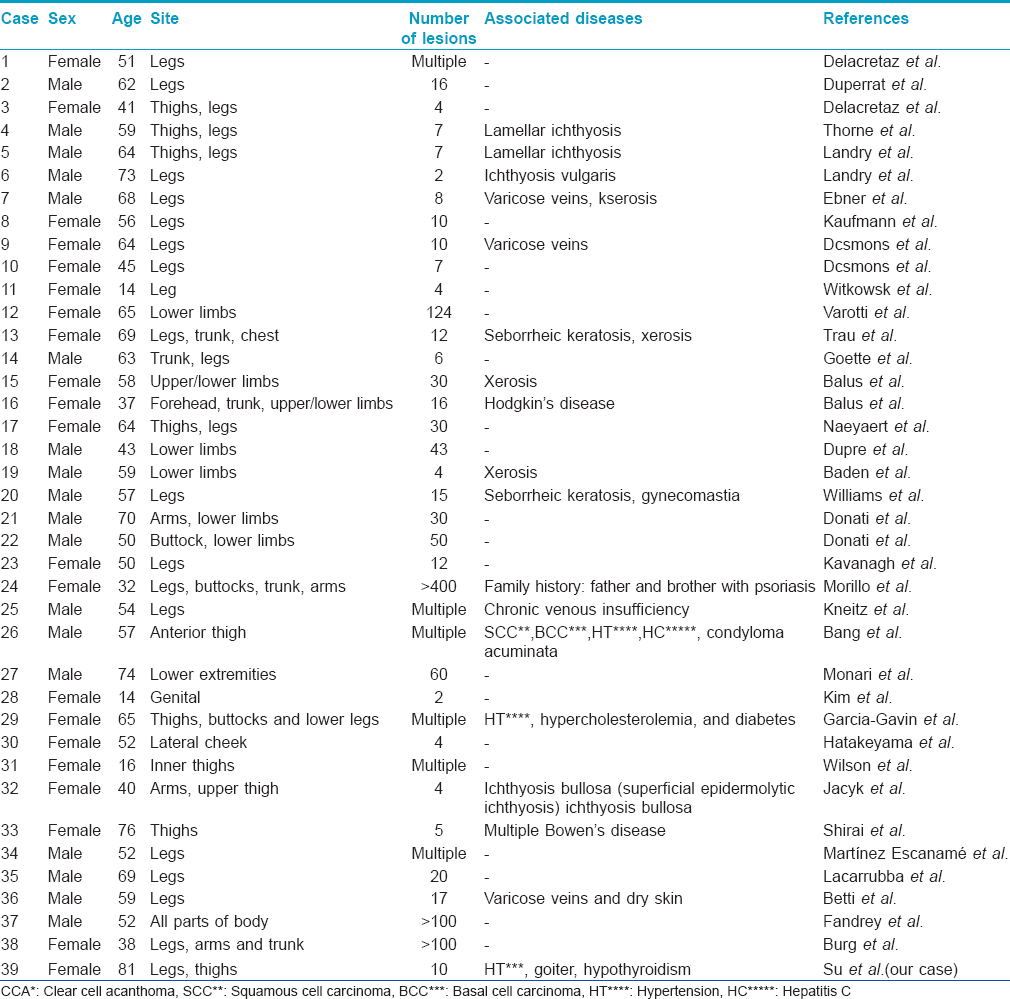
We present a case of multiple clear cell acanthomas with a giant lesion and a total of 11 lesions. We found 38 previous reports of multiple clear cell acanthoma in the literature [Table - 1]. [1],[2],[3],[4],[5],[6],[7],[8],[9],[10],[11],[12],[13],[14],[15],[16],[17],[18],[19],[20],[21],[22],[23],[24],[25],[26],[27],[28],[29],[30],[31],[32],[33],[34],[35] The most prominent associations were xerosis (6/39) and ichthyosis (4/39). Our patient had mild xerosis too.
The clinical differential diagnosis is broad and includes basal cell carcinoma, squamous cell carcinoma, Bowen′s disease, actinic keratosis, hemangioma, dermatofibroma, inflamed seborrheic keratosis, verruca vulgaris, amelanotic melanoma, psoriasis, histiocytoma, eczematous dermatitis, nevus, parapsoriasis and pyogenic granuloma. [1],[2],[3],[4],[5] Our patient had multiple red nodules with a vascular appearance. Hence, our clinical differential diagnosis was Kaposi sarcoma and B-cell lymphoma. Morrison et al. reported 411 histologically confirmed cases but noted that rarely had the condition been recognised clinically. [1] They considered that this might be due to a variable clinical appearance with overlapping features of several other lesions making it difficult to distinguish, or because it was an entity that was rare and not frequently suspected. [1]
Treatment consists of electrofulguration, curettage, surgical excision, cryotherapy, carbon dioxide laser and topical 5-fluoruracil. The most common treatment option for multiple lesions is cryotherapy, which was also performed in our patient
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
| 1. |
Morrison LK, Duffey M, Janik M, Shamma HN. Clear cell acanthoma: A rare clinical diagnosis prior to biopsy. Int J Dermatol 2010;49:1008-11.
[Google Scholar]
|
| 2. |
Ohnishi T, Watanabe S. Immunohistochemical characterization of keratin expression in clear cell acanthoma. Br J Dermatol 1995;133:186-93.
[Google Scholar]
|
| 3. |
Delacretaz J, Christeler A, Loi-Zedda P, Lenggenhager R. Acanthom a cellules claires. Dermatologica 1967;135:304.
[Google Scholar]
|
| 4. |
Langtry JA, Torras H, Palou J, Lecha M, Mascaro JM. Giant clear cell acanthoma in an atypical location. J Am Acad Dermatol 1989;21 (2 Pt 1):313-5.
[Google Scholar]
|
| 5. |
Kim CY, Kim NG, Oh CW. Multiple reddish weeping nodules on the genital area of a girl. Giant clear cell acanthoma (CCA). Clin Exp Dermatol 2010;35:e67-9.
[Google Scholar]
|
| 6. |
Martínez Escanamé M, Arzberger E, Hofmann-Wellenhof R, Massone C. Multiple clear-cell acanthomas. Australas J Dermatol 2015;56:e46-8.
[Google Scholar]
|
| 7. |
Duperrat B, Mascaro JM, Mascaro-Galy C. 7 cases of clear cell acanthoma. Arch Belg Dermatol Syphiligr 1966;22:55-9.
[Google Scholar]
|
| 8. |
Thorne EG, Fusaro RM. Multiple clear cell acanthomas in a patient with lamellar ichthyosis. Dermatologica 1971;143:105-10.
[Google Scholar]
|
| 9. |
Ebner H. Multiple clear-cell acanthomas. Z Hautkr 1974;49:541-6.
[Google Scholar]
|
| 10. |
Kaufmann J, Eichmann A, Meves C, Ott F, Somazzý ST, Storck H. Klarzellakanthom (multipel): Demonstrationen. Dermatologica 1976;153:116-7.
[Google Scholar]
|
| 11. |
Dcsmons F, Breuillard F, Thomas P, Leonardflli J, Hildebrand HF. Clear cell acanthoma (Degos). Histochemical and ultrastructural study of two cases. J Dermatol 1977;16:203-7.
[Google Scholar]
|
| 12. |
Witkowski JA, Parish LC. Clear cell acanthoma. Int J Dermatol 1979;18:162-3.
[Google Scholar]
|
| 13. |
Varotti C, Passarini B, Baratta L. Acantoma a cellule chiare multiplo. Studio istoiogico ed ultrastrutturale di un caso. G Ital Dermatol Venereol 1979;144:765-70.
[Google Scholar]
|
| 14. |
Trau H, Fisher BK, Schewach-Millet M. Multiple clear cell acanthomas. Arch Dermatol 1980;116:433-4.
[Google Scholar]
|
| 15. |
Goette DK, Diakon NC. Multiple clear cell acanthomas. Arch Dermatol 1983;119:359-61.
[Google Scholar]
|
| 16. |
Balus L, Cainelli T, Cristiani R, Donati P. Multiple familial clear cell acanthoma. Ann Dermatol Venereol 1984;111:665-6.
[Google Scholar]
|
| 17. |
Naeyaert JM, de Bersaques J, Geerts ML, Kint A. Multiple clear cell acanthomas. A clinical, histological, and ultrastructural report. Arch Dermatol 1987;123:1670-3.
[Google Scholar]
|
| 18. |
Dupre A, Viraben R. Forme eruptive de tacanthome a cellules claires. Nouv Dermatol 1987;6 Suppl 4:485.
[Google Scholar]
|
| 19. |
Baden TJ, Woodley DT, Wheeler CE Jr. Multiple clear cell acanthomas. Case report and delineation of basement membrane zone antigens. J Am Acad Dermatol 1987;16 (5 Pt 2):1075-8.
[Google Scholar]
|
| 20. |
Williams RE, Lever R, Seywright M. Multiple clear cell acanthomas - treatment by cryotherapy. Clin Exp Dermatol 1989;14:300-1.
[Google Scholar]
|
| 21. |
Donati P, Leonetti F, Paiamara G. Due casi di acantoma a cellule chiare multiplo. Dermatol Oggi 1991;5:29-31.
[Google Scholar]
|
| 22. |
Kavanagh GM, Marshman G, Burton JL. Multiple clear cell acanthomas treated by cryotherapy. Australas J Dermatol 1995;36:33-4.
[Google Scholar]
|
| 23. |
Morillo V, Manrique P, Zabalza I, Artola JL. Eruptive clear cell acanthoma. Actas Dermosifiliogr 2009;100:244-6.
[Google Scholar]
|
| 24. |
Kneitz H, Bröcker EB, Ugurel S. Slowly changing nodules on both lower limbs in a 54-year old patient. J Dtsch Dermatol Ges 2009;7:63-5.
[Google Scholar]
|
| 25. |
Bang R. Multiple clear cell acanthomas in association with hepatitis C: A novel presentation. J Am Acad Dermatol (Poster Abstracts of 68 th Annual Meeting, March 5-9, 2010 Miami, Florida) 2010;623:AB39:P1155.
[Google Scholar]
|
| 26. |
Monari P, Farisoglio C, Gualdi G, Botali G, Ungari M, Calzavara-Pinton P. Multiple eruptive clear cell acanthoma. J Dermatol Case Rep 2010;4:25-7.
[Google Scholar]
|
| 27. |
García-Gavín J, González-Vilas D, Montero I, Rodríguez-Pazos L, Pereiro MM, Toribio J. Disseminated eruptive clear cell acanthoma with spontaneous regression: further evidence of an inflammatory origin? Am J Dermatopathol 2011;33:599-602.
[Google Scholar]
|
| 28. |
Hatakeyama M, Oka M, Fukunaga A, Kunisada M, Funasaka Y, Nishigori C. A case of multiple facial clear cell acanthomas successfully treated by cryotherapy. Indian J Dermatol 2013;58:162.
[Google Scholar]
|
| 29. |
Wilson J, Walling HW, Stone MS. Benign cutaneous Degos disease in a 16-year-old girl. Pediatr Dermatol 2007;24:18-24.
[Google Scholar]
|
| 30. |
Jacyk WK, Baran W, Essop A. Multiple pigmented clear cell acanthoma in an African patient. J Eur Acad Dermatol Venereol 2014. Doi: 10.1111/jdv.12882. [Epub ahead of print].
[Google Scholar]
|
| 31. |
Shirai A, Saeki H, Matsuzaki H, Ito K, Nakagawa H. Multiple clear cell acanthoma associated with multiple Bowen′s disease. Int J Dermatol 2014;53:e386-8.
[Google Scholar]
|
| 32. |
Lacarrubba F, de Pasquale R, Micali G. Videodermatoscopy improves the clinical diagnostic accuracy of multiple clear cell acanthoma. Eur J Dermatol 2003;13:596-8.
[Google Scholar]
|
| 33. |
Betti R, Bruscagin C, Inselvini E, Palvarini M, Crosti C. Successful cryotherapic treatment and overview of multiple clear cell acanthomas. Dermatol Surg 1995;21:342-4.
[Google Scholar]
|
| 34. |
Fandrey K, Rabenhorst S, Fedler R, Frosch PJ. Multiple clear cell acanthomas. Hautarzt 1995;46:865-8.
[Google Scholar]
|
| 35. |
Burg G, Würsch T, Fäh J, Elsner P. Eruptive hamartomatous clear-cell acanthomas. Dermatology 1994;189:437-9.
[Google Scholar]
|
Fulltext Views
5,513
PDF downloads
2,250





![[Figure - 1]](#fig_ijdvl_2016_82_2_218_168913_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2016_82_2_218_168913_f2.jpg){kind=link}
![[Table - 1]](#tbl_ijdvl_2016_82_2_218_168913_t3.jpg){kind=link}