Translate this page into:
Multiple hyperpigmented patches in Waardenburg syndrome type 1: An unusual presentation
Correspondence Address:
Suresh Kumar Jain
Department of Dermatology, Venereology and Leprology, Government Medical College, Kota - 324 001, Rajasthan
India
| How to cite this article: Morgaonkar M, Gupta S, Vyas K, Jain SK. Multiple hyperpigmented patches in Waardenburg syndrome type 1: An unusual presentation. Indian J Dermatol Venereol Leprol 2016;82:711-713 |
Sir,
Waardenburg syndrome is a rare genetic disorder of neural crest cell development characterized by the association of craniofacial dysmorphisms (synophrys, telecanthus, broad and high nasal root and lower lacrimal dystopia), pigmentation defects (heterochromic and bright hypochromic blue irides, hypopigmented spots on the skin and white forelock or early graying) and sensorineural congenital hearing impairment.[1] Four variants of Waardenburg syndrome have been described. Of these, Waardenburg syndrome 1 and 2 are the most common variants and are inherited in a autosomal dominant pattern in most of the cases.
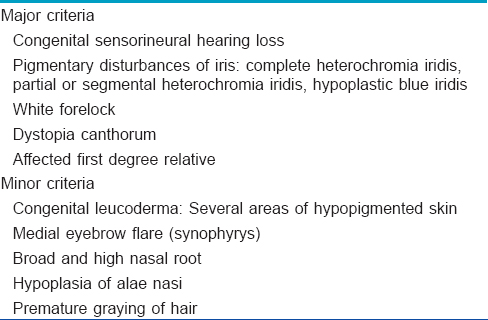
Leukoderma (hypopigmented patches) is a characteristic feature of Waardenburg syndrome and hence is included in the widely accepted diagnostic criteria proposed by the Waardenburg consortium [Table - 1].[2] We report a case of Waardenburg syndrome 1, having a predominance of multiple hyperpigmented patches all over the body along with only a few hypopigmented patches.
A 9-month-old boy, the first child of a non-consanguineous marriage, was born following a full-term uncomplicated vaginal delivery and presented with a white forelock and multiple brown colored areas all over the body since birth. There were two first-trimester abortions in the mother prior to this pregnancy. Family history was not contributory. The child was active and feeding well.
Clinical examination revealed a white forelock (poliosis) in the frontal area with an underlying depigmented patch [Figure - 1]a. There were multiple, ill-defined, dark brown, hyperpigmented patches ranging from 0.5 cm to 7 cm all over the body, relatively sparing the face [Figure - 2]. In addition, a few ill-defined hypopigmented patches with islands of hyperpigmentation within them were noted on the lower abdomen and thighs [Figure - 3]. The nasal root was broad. On ophthalmological examination, dystopia canthorum and bilaterally blue iridis were found [Figure - 1]b. Systemic examination including cardiovascular and orthopedic examination was normal and routine laboratory investigations including complete blood count, liver and kidney function tests, chest X-ray, electrocardiogram and echocardiography were normal. Brainstem evoked response audiometry revealed bilateral sensorineural hearing loss. Physical development and milestones were appropriate for age.
 |
| Figure 1: (a) White forelock, (b) closer view showing broad nasal root, dystopia canthorum and bilateral blue irides |
 |
| Figure 2: (a) Hyperpigmented and some hypopigmented patches all over body, (b) hyperpigmented and hypopigmented patches on buttocks and posterior aspect of thighs |
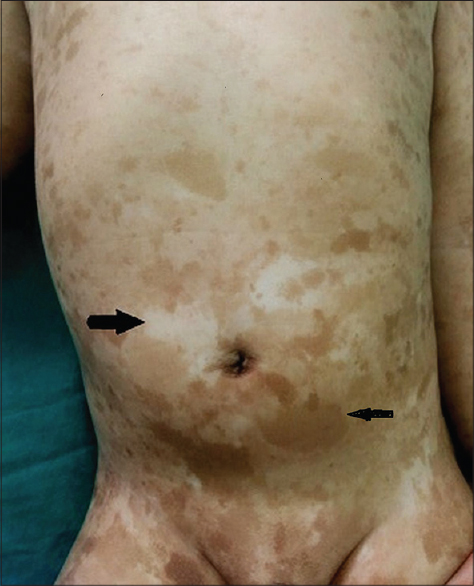 |
| Figure 3: Close up view of lesions on abdomen |
The diagnosis of Waardenburg syndrome 1 was made as per the Waardenburg Consortium criteria. Owing to the presence of multiple hyperpigmented patches, conditions such as LEOPARD syndrome and neurofibromatoses were considered as differential diagnoses but were subsequently ruled out on the basis of clinical examination and relevant investigations.
Waardenburg syndrome was first described by P. J. Waardenburg in 1951. The incidence in the normal population is around 1/42,000.[3] Subtypes of this heterogenous disorder are described as type 1, type 2, Klein's syndrome (type 3) and Shah-Waardenburg syndrome (type 4).
Waardenburg syndrome 1, which is one of the most common subtypes, is caused by mutations in the PAX3gene (2q35), a transcription factor for the microphthalmia-associated transcription factor gene, which in turn activates a number of genes associated with melanogenesis such as those encoding tyrosinase as well as those mediating survival of melanocytes through Bcl-2. The PAX transcription factor is the key component in neural crest differentiation, melanoblast activation, melanoblast migration and in the development of facial bones, facial cartilage and the inner ear. The syndrome has variable penetrance and expression. Sporadic cases have also been reported.
The most frequent cutaneous pigmentary abnormality in Waardenburg syndrome 1 is the white forelock (17–58.4% of patients) followed by white macules that are anatomically distinct from the white forelock (in approximately15% of patients).[4]
Our patient fulfills the diagnostic criteria of Waardenburg syndrome 1 but with the additional presence of multiple hyperpigmented patches which do not form a part of the Waardenburg consortium criteria. Nork et al.[5] in 1986 reported a case of Waardenburg syndrome 2 with two discrete hyperpigmented macules on the eyelid and sacrum. Although islands of hyperpigmentation within the achromatic patches has been reported frequently, our patient has the distinctive feature of concurrent presence of multiple large hyperpigmented patches all over the body. It may be attributed to the fact that Waardenburg syndrome occurs due to aberrant development and/or migration of melanocyte precursors to epidermis. We were unable to find any previous reports of a similar presentation in a case of Waardenburg syndrome type 1.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the legal guardian has given his consent for images and other clinical information to be reported in the journal. The guardian understands that names and initials will not be published and due efforts will be made to conceal patient identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
| 1. |
Pardono E, Mazzeu JF, Lezirovitz K, Auricchio MTBM, Iughetti P, Nascimento RMP, et al. Waardenburg syndrome: Description of two novel mutations in the PAX3 gene, one of which incompletely penetrant. Genet Mol Biol 2006;29:601-4.
[Google Scholar]
|
| 2. |
Farrer LA, Grundfast KM, Amos J, Arnos KS, Asher JH Jr., Beighton P, et al. Waardenburg syndrome (WS) type I is caused by defects at multiple loci, one of which is near ALPP on chromosome 2:First report of the WS consortium. Am J Hum Genet 1992;50:902-13.
[Google Scholar]
|
| 3. |
Kiani R, Gangadharan SK, Miller H. Association of Waardenburg syndrome with intellectual disability, autistic spectrum disorder and unprovoked aggressive outbursts: A new behavioural phenotype? Br J Dev Disabil 2007;53:53-62.
[Google Scholar]
|
| 4. |
Reed WB, Stone VM, Boder E, Ziprkowski L. Pigmentary disorders in association with congenital deafness. Arch Dermatol 1967;95:176-86.
[Google Scholar]
|
| 5. |
Nork TM, Shihab ZM, Young RS, Price J. Pigment distribution in Waardenburg's syndrome: A new hypothesis. Graefes Arch Clin Exp Ophthalmol 1986;224:487-92.
[Google Scholar]
|
Fulltext Views
3,173
PDF downloads
1,480





![[Table - 1]](#tbl_ijdvl_2016_82_6_711_188657_t4.jpg){kind=link}
![[Figure - 1]](#fig_ijdvl_2016_82_6_711_188657_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2016_82_6_711_188657_f2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2016_82_6_711_188657_f3.jpg){kind=link}