Translate this page into:
Multiple minute digitate hyperkeratosis, familial type: A rare entity
Correspondence Address:
Siva Rami Reddy Karumuri
Department of DVL, Bhaskar Medical College, Yenkapally, Moinabad, Ranga Reddy, Hyderabad, Telangana
India
| How to cite this article: Karumuri SR, Surampally SL, Reddy V S, Thambisetti NB. Multiple minute digitate hyperkeratosis, familial type: A rare entity. Indian J Dermatol Venereol Leprol 2020;86:63-65 |
Sir,
A 35-year-old woman presented to the Dermatology Department of Bhaskar Medical College, Telangana, India, with cutaneous lesions resembling minute finger-like projections on the trunk and limbs since 25 years. These lesions were insidious in onset and progressed to involve different parts of the body. Similar lesions were noticed near the medial canthi of both eyes since 2 years. The patient had no history of any nutritional deficiency, inflammatory skin disease, or malignancy. There was no history of exposure to radiation, topical application or ingestion of any drug, and no immunosuppression. Her medical history was unremarkable. She had no other complaints. There was a positive family history of similar lesions in her 10 year old daughter over the trunk and limbs.
The patient's cutaneous examination revealed multiple, asymptomatic, symmetrically distributed, skin-colored to slightly yellowish, keratotic, finger-like projections of approximately 1–5 mm in length and 1–2 mm in width. The lesions were located on the extensor aspects of both upper arms, forearms, elbows [Figure - 1], gluteal region [Figure - 2], lateral thighs, knees, posterior axillary folds, lateral trunk, and also involved the posterior scalp hairline. Crops of such lesions were seen near the medial canthi of both eyes [Figure - 3]. The palms and soles were not involved. There was no clinical evidence suggestive of nutritional deficiency. On examination, her daughter had similar non-follicular, spiky lesions over both elbows [Figure - 4].
 |
| Figure 1: Spiky keratotic projections over the elbow of the mother |
 |
| Figure 2: Spiky keratotic projections over the gluteal area of the mother |
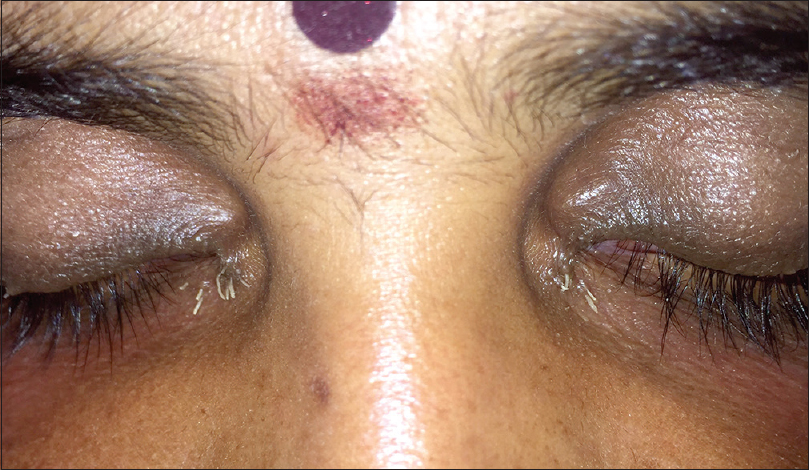 |
| Figure 3: Spiky keratotic projections near the inner canthus of both eyes of the mother |
 |
| Figure 4: Spiky keratotic projections over the elbow of the child |
Histological examination of the lesional skin showed non-follicular, dome-shaped or oblique columns of orthokeratotic hyperkeratosis with a compact stratum corneum and acanthosis. The stratum granulosum appeared diminished in thickness. The epidermis between the columns was unremarkable. The upper dermis showed a mild lymphocytic infiltrate around the vessels. The deeper dermis was normal [Figure - 5]. Other investigations included complete blood count, complete urine examination, serum vitamin A levels, liver function tests, renal function tests, serum electrolytes, chest X-ray, and abdominal sonography, which were all within normal limits.
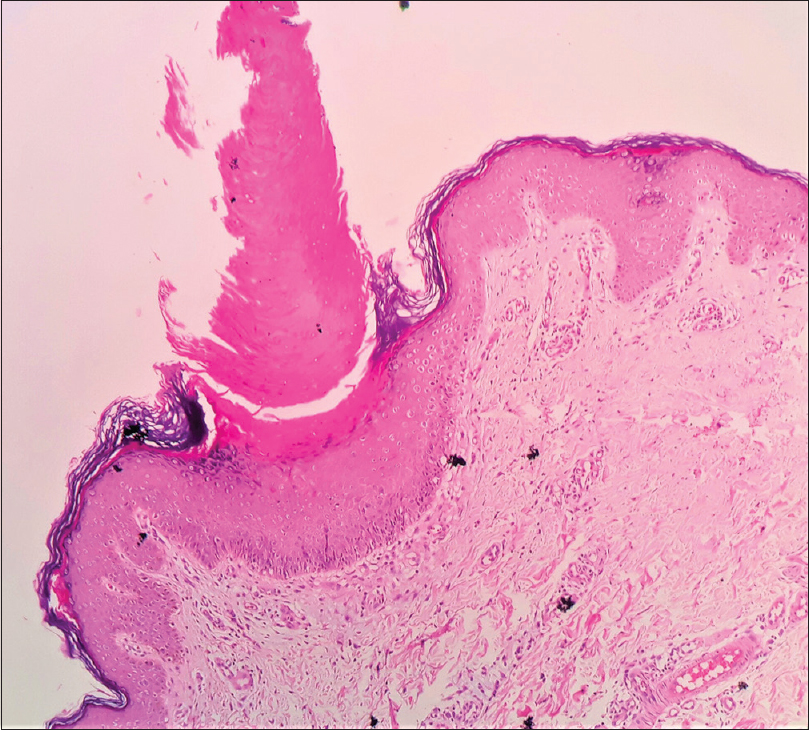 |
| Figure 5: Epidermis shows two distinct oblique columns of orthokeratosis seen as a spike with absent granular layer below. Few scattered dyskeratotic keratinocytes (H and E, ×400) |
The diagnosis of multiple minute digitate hyperkeratosis of familial type was made, based on asymptomatic generalized, non-follicular distribution of keratotic papules with spiky projections, positive family history of similar lesions, corroboratory histopathology, absence of both nutritional deficiency and evidence of malignancy.
The patient was treated with topical salicylic acid, urea, propylene glycol, and emollients twice daily and oral isotretinoin 0.25 mg/kg body weight at night. The child was treated with topical creams and oral vitamin A supplements. The lesions healed after a few months in both the mother and the child but reappeared after stopping treatment.
Multiple minute digitate hyperkeratosis is a term coined by Goldstein in 1967.[1] It is an unusual disorder of keratinization of unknown etiology.[1] This disorder is synonymous with digitate keratoses, disseminated spiked hyperkeratosis, minute aggregate keratoses, familial disseminated filiform hyperkeratosis, and spiny hyperkeratosis.[2] The clinical hallmark of this disease is the presence of multiple asymptomatic skin-colored small spiky projections in a follicular or nonfollicular distribution, and flat-topped to dome shaped keratotic papules usually located on the trunk and limbs.[3] In our case, multiple spiny digitate projections which were grouped and symmetrical were also seen near the inner canthus of both eyes. Its pathogenesis remains unknown.[3] Proposed etiopathogenesis for the familial form, which is inherited as an autosomal dominant trait, includes drugs like etretinate, and exposure to radiation or arsenic. Microscopically, multiple minute digitate hyperkeratosis is characterized by digitiform orthohyperkeratosis with mild acanthosis and elongation of rete ridges, normal or slightly diminished stratum granulosum, and a mild lymphocytic infiltrate of the upper dermis.[3]
Multiple minute digitate hyperkeratosis is a new chronic disturbance of keratinization, clinically and histologically distinct from other disorders in the spectrum such as lichen spinulosus, phrynoderma, follicular lichen planus, and porokeratosis.[3],[4]
Lichen spinulosus mainly occurs in children and young adults, and presents as grouped follicular papules and plaques with pointed keratotic spines, symmetrically distributed on the trunk, buttocks, neck, knees, and elbows sparing face, hands, and feet.
Phrynoderma is a cutaneous manifestation of vitamin A deficiency which is commonly seen in pre-adolescent children and manifests as follicular hyperkeratosis with central keratotic plug over the elbows, knees, buttocks, and extensors of limbs. This condition is sometimes associated with ocular signs such as night blindness and conjuctival xerosis.
Follicular lichen planus is associated with typical lichen planus lesions. Follicular lesions on the scalp are accompanied by scaling and are a cause of scarring alopecia. It shows a remarkable female preponderance.
Various classification systems have been proposed, of which the classification proposed by Ramselaar and Toonstra in 1999 rightly represents the whole clinic-pathological spectrum of multiple minute digitate hyperkeratosis.[3]
According to their guidelines, we can distinguish early and late-onset multiple minute digitate hyperkeratosis.
(1) The early-onset form manifests in the second to third decades of life, may be hereditary as an autosomal dominant inheritance or acquired, and is generalized in distribution predominantly nonfollicular and (2) the late-onset form is sporadic, occurs in middle age, presents as a follicular or nonfollicular pattern, and may act as the presenting sign of a malignant or nonmalignant concomitant disease.
Benoldi et al. classified the disease into three distinct types: familial, sporadic, and postinflammatory.[5]
Our patient is an example of the early-onset, familial form of digitate hyperkeratosis.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patient has given her consent for her images and other clinical information to be reported in the journal. The patient understand that name and initials will not be published and due efforts will be made to conceal identity, but anonymity cannot be guaranteed.
Acknowledgement
The authors thank Dr. P. Sridevi, MD, Consultant Dermatopathologist, Dermpath Institute and Research Centre, Hyderabad, India, and Dr. V. Vijay Sreedhar, Professor and HOD, Department of Pathology, Bhaskar Medical College, Yenkapally, Ranga Reddy Dt, Telangana State, India.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
| 1. |
Goldstein N, Multiple minute digitate hyperkeratosis. Arch Dermatol 1967;96:692-3.
[Google Scholar]
|
| 2. |
Shuttleworth D, Graham-Brown RA, Hutchinson PE. Minute aggregate keratosis – A report of three cases. Arch Dermatol 1985;10:566-71.
[Google Scholar]
|
| 3. |
Ramselaar C, Toonstra J. Multiple minute digitate hyperkeratosis: Report of two cases with an updated review and proposal for a new classification. Eur J Dermatol 1999;9:460-5.
[Google Scholar]
|
| 4. |
Mueller KK, Yeager JK. Clinical considerations in digitatedermatosis. Int J Dermatol 1997;36:767-8.
[Google Scholar]
|
| 5. |
Benoldi D, Zucchi A, Allegra F. Multiple minute digitate hyperkeratosis. Clin Exp Dermatol 1993;18:261-2.
[Google Scholar]
|
Fulltext Views
12,440
PDF downloads
2,326





![[Figure - 1]](#fig_ijdvl_2020_86_1_63_271700_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2020_86_1_63_271700_f2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2020_86_1_63_271700_f3.jpg){kind=link}
![[Figure - 4]](#fig_ijdvl_2020_86_1_63_271700_f4.jpg){kind=link}
![[Figure - 5]](#fig_ijdvl_2020_86_1_63_271700_f5.jpg){kind=link}