Translate this page into:
Multiple subcutaneous angiomyxolipomas associated with olecranon bursa cyst: A rare presentation of a rare entity
2 Department of Surgery, Smt. Kashibai Navale Medical College and General Hospital, Narhe, Pune, Maharashtra, India
Correspondence Address:
Mani Anand
Department of Pathology, Smt. Kashibai Navale Medical College and General Hospital, Narhe, Off Pune-Mumbai Bypass, Pune - 411 041, Maharashatra
India
| How to cite this article: Anand M, Deshmukh SD, Gulati HK, Yadav PR. Multiple subcutaneous angiomyxolipomas associated with olecranon bursa cyst: A rare presentation of a rare entity. Indian J Dermatol Venereol Leprol 2012;78:204-206 |
Sir,
Angiomyxolipoma is a rare benign mesenchymal tumor. We describe this lesion in an 81-year-old male who presented with a gradually increasing painless swelling over the right elbow for the past 2 years following a trivial trauma. On local examination, a 6 cm × 4 cm soft, cystic, fluctuant, mobile, non-tender mass was seen at the posterior aspect of the right elbow. It was clinically diagnosed as olecranon bursa cyst. Also, multiple, discrete, tiny, soft, granular lesions were palpated in the subcutaneous tissue adjacent to the cyst. The cyst, along with the granular lesions, were excised. On gross examination, the specimen consisted of a 5 cm × 3 cm × 0.5 cm cystic mass filled with serous fluid. The external surface showed tiny elevated yellowish nodules [Figure - 1]a. Also received were multiple soft encapsulated gelatinous yellowish nodular masses ranging in size from 0.5 to 1 cm in largest dimension [Figure - 1]b. Histopathological examination of the cyst revealed a flattened lining epithelium. The cyst wall was comprised of fibrocollagenous tissue along with few congested blood vessels. Also seen within the cyst wall were well-demarcated nodular lesions comprised of an admixture of mature adipocytes, blood vessels and myxoid areas [Figure - 2]a and b. Microscopic examination of the multiple tiny nodular masses revealed a multilobular tumor surrounded by a fibrous capsule and comprising of mature adipocytes along with numerous thin- and thick-walled blood vessels with periadventitial myxoid stroma [Figure - 2]c and d. There was no evidence of cytological atypia, mitoses or necrosis. Lipoblasts were not seen. Patchy perivascular lymphocytic infiltrate was seen at places. The myxoid stroma stained positively for Alcian blue [Figure - 3]. The endothelial cells lining the vascular lumen and the cellular component of the myxoid stroma were immunoreactive for CD34 and vimentin, whereas the adipocytes were reactive for vimentin and focally for S-100 [Figure - 4]a and b. The spindle cells in the myxoid areas did not express desmin, smooth muscle actin, HMB-45 or S-100. Based on the above features, a diagnosis of multiple subcutaneous angiomyxolipomas associated with olecranon bursal cyst was offered. The patient is symptom-free without any recurrence after a 6-month follow-up.
 |
| Figure 1: (a) A 5 cm × 3 cm × 0.5 cm cystic mass with tiny elevated yellowish nodules on the external surface. (b) Multiple soft encapsulated gelatinous yellowish nodular masses ranging in size from 0.5 to 1 cm |
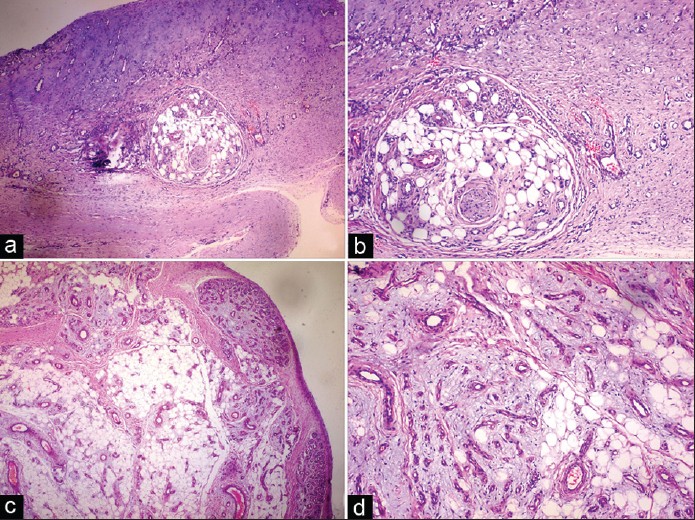 |
| Figure 2: (a and b) Microscopy of the cyst wall showing fibrocollagenous tissue, congested blood vessels and well-demarcated nodular lesions comprised of an admixture of mature adipocytes, blood vessels and myxoid areas (a, H and E, × 40; b, H and E, × 100). (c and d) PhotomicroGraph of the multiple tiny nodular masses revealing a multilobular tumor surrounded by a fibrous capsule and comprising of mature adipocytes along with numerous thin- and thick-walled blood vessels with periadventitial myxoid stroma (c, H and E, × 40; d, H and E, × 100) |
 |
| Figure 3: The myxoid stroma staining positively for Alcian blue (× 100) |
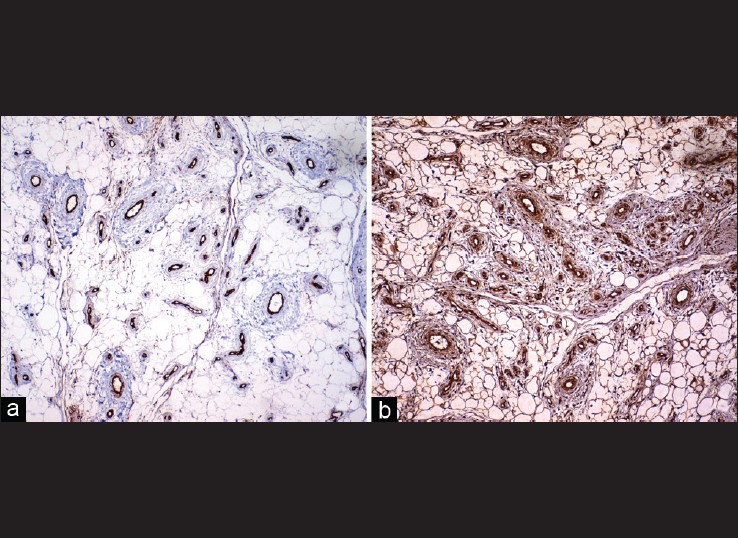 |
| Figure 4: Immunohistochemical reactivity for CD34 in endothelial cells and cellular component of the myxoid stroma (a, × 100) and vimentin in adipocytes, endothelial cells and the cellular component of the myxoid stroma (b, × 100) |
Angiomyxolipoma was first described by Mai et al. [1] It is a rare variant of lipoma, with very few cases being reported in the literature. The patients′ ages ranged from 32 to 69 years, with a male preponderance. The duration of symptoms can range from 3 months to 7 years. [2] The most common location has been the subcutaneous tissue, in the scalp, arm, wrist, thigh and the gluteal region; [2] with occasional cases being located in the spermatic cord, subungual and intra-articular region. [1],[3],[4] It usually presents as a solitary, mobile, well-demarcated, non-encapsulated subcutaneous mass with a yellow gelatinous cut-surface. [1],[2],[3] The lesion may be associated with pain, owing to its increased vascularity. In contrast, simple lipomas are encapsulated painless rounded masses with a pale yellow to orange color with a uniform greasy surface and an irregular lobular pattern. [5] Computed tomography of lipoma reveals a mass having the appearance of subcutaneous fat with a more uniform density than liposarcomas. On magnetic resonance imaging (MRI), both benign and malignant lipomatous tumors exhibit a high signal intensity on TI-weighted images. [5] MRI of angiomyxolipoma shows heterogeneous mass with mixed signal intensity on T2-weighted images. [4] To our knowledge, this is the first case of multiple angiomyxolipomas associated with an olecranon bursa cyst. Excision is the treatment of choice. The differential diagnosis includes variants of lipomas, such as myxolipoma, angiolipoma, angiomyolipoma, superficial angiomyxoma, myxoid spindle cell lipoma and myxoid liposarcoma and low-grade myxofibrosarcoma. [2] Both myxolipoma and angiolipoma lack one of the three major components of angiomyxolipoma, and angiomyolipoma displays bundles of smooth muscle cells. Superficial angiomyxoma is a poorly circumscribed mass of adipose tissue accompanied by epithelial structures and a mixed inflammatory infiltration of neutrophils. Myxoid spindle cell lipoma lacks ropy collagen and has poor vascularity, which differentiate it from angiomyxolipoma. [2] Absence of lipoblasts and a diffuse capillary plexiform pattern is against myxoid liposarcoma. [5] To conclude, histopathologic findings showing a mixture of adipose tissue, myxoid stroma and abundant blood vessels without immature or atypical cells should suggest to dermatologists and pathologists a diagnosis of angiomyxolipoma with its benign nature. [2]
| 1. |
Mai KT, Yazdi HM, Collins JP. Vascular myxolipoma ("angiomyxolipoma") of the spermatic cord. Am J Surg Pathol 1996;20:1145-8.
[Google Scholar]
|
| 2. |
Song M, Seo SH, Jung DS, Ko HC, Kwon KS, Kim MB. Angiomyxolipoma (vascular myxolipoma) of subcutaneous tissue. Ann Dermatol 2009;21:189-92.
[Google Scholar]
|
| 3. |
Sanchez Sambucety P, Alonso TA, Agapito PG, Moran AG, Rodriguez Prieto MA. Subungual angiomyxolipoma. Dermatol Surg 2007;33:508-9.
[Google Scholar]
|
| 4. |
Bergin PF, Milchteim C, Beaulieu GP, Brindle KA, Schwartz AM, Faulks CR. Intra-articular knee mass in a 51-year-old woman. Orthopedics 2011;34:223-9.
[Google Scholar]
|
| 5. |
Weiss SW, Goldblum JR. Benign lipomatous tumors. In: Weiss SW, Goldblum JR, editors. Soft tissue tumors. 5 th ed. Philadelphia: Mosby, Elsevier; 2008. p. 431-4.
[Google Scholar]
|
Fulltext Views
3,080
PDF downloads
1,875





![[Figure - 1]](#fig_ijdvl_2012_78_2_204_93649_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2012_78_2_204_93649_f2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2012_78_2_204_93649_f3.jpg){kind=link}
![[Figure - 4]](#fig_ijdvl_2012_78_2_204_93649_f4.jpg){kind=link}