Translate this page into:
Nails in systemic disease
Correspondence Address:
Gurcharan Singh
108, A, Jal Vayu Vihar, Kammanahalli, Bangalore - 560 043
India
| How to cite this article: Singh G. Nails in systemic disease. Indian J Dermatol Venereol Leprol 2011;77:646-651 |
Abstract
Nail abnormalities secondary to systemic disease could be classified as nail abnormalties associated with systemic disease, disease of specific organ system or associated with syndromes and genodermatoses. Because nail findings are easily observable and yield valuable information, careful examination of nails could be an important diagnostic tool for a dermatologist. A brief review of the common and not so common nail changes in systemic illness is presented.Introduction
Nail abnormalities can be a revealing sign of a systemic disease. Nail plate and nail unit abnormalities may be helpful as diagnostic tools or as a part of the puzzle for confirmation of a systemic disease. There are specific and nonspecific nail signs, which can be seen involving one or more nails, that occur simultaneously or secondary to systemic disease. Occasionally these clues can be diagnostic. Understanding a nail abnormality will aid in avoiding incorrect and expensive diagnostic work up and treatment.
Classification
Nail abnormalities in systemic disease can be broadly classified as follows. [1]
- Nail abnormalities less specifically associated with systemic disease
- Splinter hemorrhages.
- Beau′s lines.
- Onycholysis.
- Pitting.
- Koilonychia.
- Pigmented bands.
- Anonychia
- Micronychia
- Nail abnormalities more specifically associated with systemic disease
- True leukonychia - Mee′s lines (arsenic poisoning)
- Apparent leukonychia - Muehrcke′s lines (hypoalbuminemia), half and half nails (renal disease), Terry′s nails (hepatic cirrhosis).
- Clubbing - Cardiopulmonary disease.
- Nail abnormalities associated with disease of a specific organ system
- Renal disease
- Pulmonary disease
- Gastrointestinal disease
- Cardiovascular disease
- Endocrine disease
- Autoimmune disease
- Infectious disease
- Central and peripheral nervous system disease
- Psychological disease
- Miscellaneous disease
- Nail abnormalities associated with specific syndromes or genodermatoses (described later in the text)
I. Nail Abnormalities Less Specifically Associated with Systemic Disease
Splinter hemorrhages
These linear brown-black or red streaks in the basal nail plate result from extravasation of blood from the longitudinally oriented vessels of the nail bed. [1] Trauma is the most common cause but subacute bacterial endocarditis is by far the commonest systemic cause. [2] Simultaneous appearance of splinter hemorrhages in multiple nails are more likely to indicate an underlying systemic disease. Few other systemic causes include rheumatoid arthritis, internal malignancy, mitral stenosis and systemic lupus erythematosus, antiphospholipid syndrome, peptic ulcer disease, malignancies, oral contraceptive use, pregnancy, psoriasis, trauma. [3] They move distally with the growth of the nail. [2]
Beau′s lines
These are transverse depressions in the nail plate that occur after a stressful event that temporarily interrupts nail formation. [4] They appear first at the cuticle and move distally with nail growth. Beau′s lines are more apparent on thumb and great toe nails. They have a margin parallel to the lunula, when caused by a systemic disease. The time of stress can be calculated after measuring the distance from the cuticle to the Beau′s lines. [5],[6] Width of the furrow indicates duration of the illness. [1] Beau′s lines have been described in systemic disorders like coronary thrombosis, measles, mumps, Kawasaki′s disease, pneumonia, pulmonary embolism, and renal failure. [5]
Onycholysis
A distal and / or lateral separation of the nail plate from the nail bed is called onycholysis. [7] Onycholysis can be classified as primary (idiopathic) and secondary. Overzealous manicure, frequent wetting, and cosmetic solvents may be the cause of primary onycholysis. [8] The systemic causes of secondary onycholysis include yellow syndrome, bronchogenic carcinoma, anemia, diabetes mellitus, pregnancy connective tissue disease, porphyrias, shell nail syndrome, and peripheral vascular disease. [9] In thyrotoxicosis, nails are undulated and curved upwards. They are called Plummer′s nails and are commonly seen in 4 th or 5 th finger nail. [1]
Anonychia
Anonychia describes permanent failure of the nail plate development, which may be complete or partial (micronychia). They can be seen in deafness, onychodystrophy, osteodystrophy and mental retardation (DOOR) syndrome, ectodermal dysplasias, Iso-Kikuchi syndrome and nail patella syndrome. [10]
Koilonychia
Reverse curvature in the transverse and longitudinal axes giving a concave dorsal aspect to the nail is called koilonychia (spoon shaped nails). The features are most prominent in the thumb or great toe. The most common causes are iron deficiency anemia and hemochromatosis. [11] Other systemic causes include coronary artery disease, upper gastrointestinal (GI) carcinoma and hypothyroidism. [1]
Pitting
Pitting is punctate depressions in the nail plate. It may be caused by a variety of systemic diseases, including Reiter′s syndrome, sarcoidosis, incontinentia pigmenti, and other connective tissue disorders. [3]
II. Nail Abnormalities More Specifically Associated with Systemic Disease
Leukonychia (White nails)
There are several types of leukonychia
- True leukonychia (pathology originates in the matrix and emerges in the nail plate).
- Apparent leukonychia (pathology is in the nail bed).
- Pseudoleukonychia (nail plate pathology is exogenous).
a. True leukonychia
True leukonychia can be total, subtotal, or partial (Transverse, punctate, longitudinal most commonly). Total leukonychia is rare and inherited and is porcelain white. In subtotal leukonychia, proximal two-thirds are white becoming pink distally. Transverse and punctate forms are commonly forms of partial leukonychia. [12]
Mee′s nail is characterized by a single, transverse, narrow whitish line that runs the width of the nail plate and is seen on multiple nails. Arsenic intoxication is a classically known cause of Mee′s lines. These tend to be single but may also manifest as multiple transverse lines. The lines do not disappear on blanching. They are also found in Hodgkin′s disease, congestive heart failure (CHF) patients, and patients with carbon monoxide poisoning. [10],[13]
b. Apparent leukonychia
Several patterns of apparent leukonychia have been described.
- Muehrcke′s lines
- Half and half (Lindsay′s) nails
- Terry′s nails
Muehrcke′s lines
These are double white transverse lines that represent an abnormality of the nail vascular bed. They disappear temporarily on squeezing the distal digit. They usually occur on the 2 nd , 3 rd , and 4 th fingernails. Chronic hypoalbuminemia is a common cause and Muehrcke′s lines disappear on serum albumin levels of 2.2g/100 ml. [6] Conditions causing hypoalbuminemia like nephrotic syndrome and glomerulonephritis are implicated. Liver disease, chemotherapeutic drugs, and malnutrition can also be responsible. [10] Muehrcke′s lines have been reported in association with heart transplantation [6] and Peutz Jegher′s syndrome. [14] Muehrcke′s bands may be confused with Mee′s lines, the difference being that they resolve with normalization of the serum albumin and do not grow out distally. [15]
Half and half nails
Half and half or Lindsay′s nails [Figure - 1] are a form of apparent leukonychia with a normal proximal half and a distinctly abnormal brownish distal portion. [16] The distal portion begins proximally where the normal or whitish nail ends and terminates distally where the free end of the nail loses its attachment to the hyponychium. They have been detected in the uremic chronic renal failure patients. [10],[15]
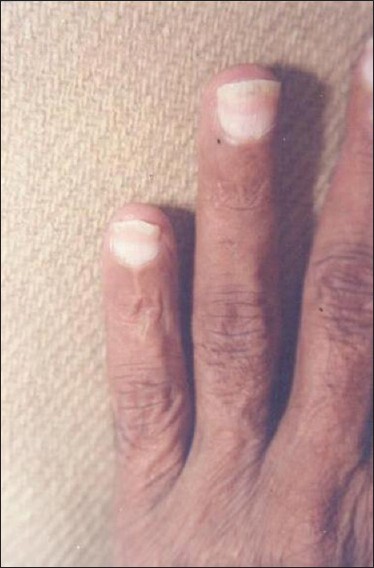 |
| Figure 1: Half and half nails |
Terry′s lines
This is white proximally and normal distally and can also be seen in normal subjects. It is attributed to cirrhosis mainly, and also in congestive cardiac failure, adult onset diabetes mellitus, peripheral vascular disease, hemodialysis patients, renal transplant patients, and HIV patients. [10],[17] Most of the nail plate turns white with the appearance of ground glass and the lunula is obliterated [Figure - 2].
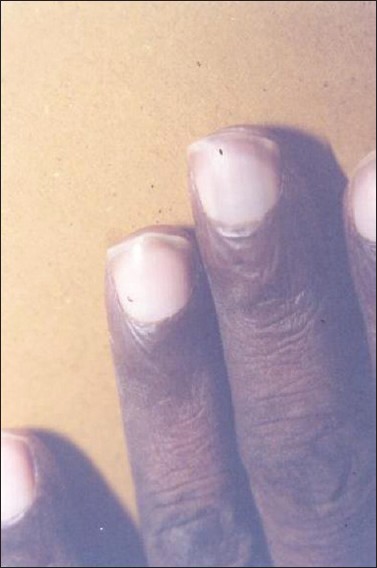 |
| Figure 2: Terry's nails |
c. Clubbing
The characteristic features of clubbing are increased nail plate curvature in both directions and soft tissue hypertrophy of the digital pulp and nail bed dermis [Figure - 3]. All 20 digits are usually affected; however, early stages can present with unilateral clubbing or prominent bi-directional over curvature of the three radial fingers. [15]
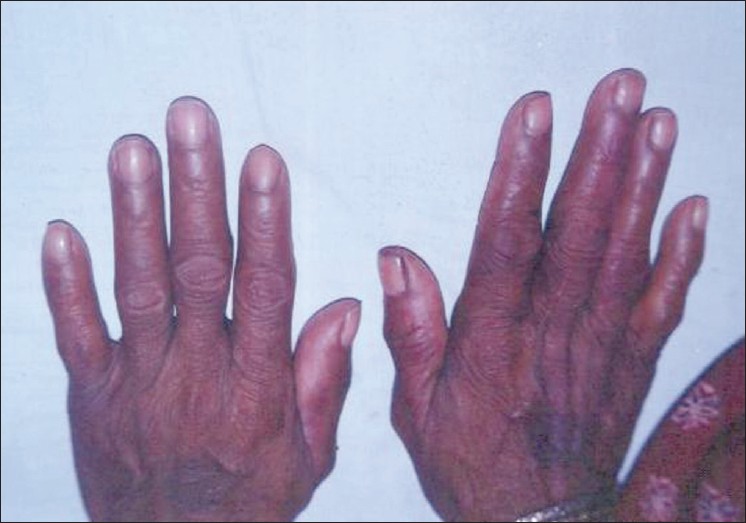 |
| Figure 3: Nail clubbing |
Clubbing occurs in diseases as different as Crohn′s disease, ulcerative colitis, biliary cirrhosis, primary hypertrophic osteoarthropathy, cystic fibrosis and cancer of the esophagus. [18] The angle between the finger proximal to the nail and the proximal nail plate is straightened, creating the "Schamroth sign," which is an obliteration of the normally diamond-shaped space formed when dorsal sides of the distal phalanges of corresponding right and left digits are opposed. [16]
III. Nail Abnormalities Associated with Disease of a Specific Organ System
Renal system
Half and half nails are seen in chronic renal failure patients. Terry′s nails can be seen in renal transplant patients. Multiple splinter hemorrhages can be seen in patients on hemodialysis. Muehrcke′s lines are seen in hypoalbuminemia which is commonly associated with nephrotic syndrome. Mee′s lines, splinter hemorrhages and Muehrcke′s lines have all been associated with renal failure. In nail patella syndrome, the accompanying renal failure presents with nail dystrophy, triangular lunula, longitudinal ridging and koilonychia. Renal adenocarcinoma may manifest with increased reddish colour of the nail bed due to production of erythropoietin. [6],[18]
Pulmonary disease
Yellow nail syndrome is characterized by a triad of yellow nails, lymphoedema and respiratory tract involvement, with or without sinusitis. Nail changes include thick, yellow nails, with increased transverse curvature, loss of cuticle associated with a rounded proximal nail-fold and slowed growth rate. [19] The yellow nail syndrome is associated with many pulmonary diseases like asthma, pleural effusion, tuberculosis, bronchiectasis, chronic sinusitis, chronic bronchitis, and chronic obstructive pulmonary disease. [6],[20]
Gastrointestinal disease
The presence of onychomycosis in addition to plantar and inter-digital mycoses is seen in patients with primary biliary cirrhosis. The most common finding reported in liver cirrhosis patients is Terry′s nails. Longitudinal striations, dystrophic nails, brittle nails, onychorrhexis and true leukonychia can be found in hepatitis B and hepatitis C. [21] Bluish lunula have been observed in Wilsons disease and in hemochromatosis, where in a blackish pigment, presumably melanin, appears on the nails. [18] Nails are white, brittle, and often triangular in Crockhite-Canada syndrome. [6]
Cardiovascular system
Splinter hemorrhages are seen in endocarditis and patients with arterial emboli. Coronary disease can present with koilonychias. Red lunula is often seen in congestive cardiac failure. [6] Nail shedding can occur with Kawasaki′s disease. [1]
Hemotologic system
Hemorrhages under the nail plate are found in leukemic patients and in those with bleeding diatheses. [18] Patients with hemochromatosis present with gray, blue or brown nails; leukonychia and longitudinal striations.
Endocrine system
Longitudinal pigmented bands occur in nails of patients with Addison′s disease and also in patients who have undergone bilateral adrenalectomy for Cushing′s disease. Patients with acromegaly present with short, wide and brittle nails. [6] Periungual erythema and telangiectasia can be seen in the nail folds as an early finding of diabetes. Over time, many diabetics develop nails that are yellow, thickened, and sometimes fragile, ridged, and brittle. The nail changes seen with hyperthyroidism are subtle and usually consist of onycholysis beginning in the fourth or fifth nail, the so-called Plummer′s nails. [22]
Infectious disease
Syphilis has been associated with elkynosis, paronychia, onychomadesis, fragility and racket nails. Leprosy may manifest with leukonychia, painful subungual abscess, lilac line of Milan and pterygium unguium. Reddish lunulae have been reported in lymphogranuloma venereum, and gray nails in patients with malaria. [1] Patients with acquired immunodeficiency syndrome may have yellowing of nails, longitudinal melanonychia, splinter hemorrhages, transverse and longitudinal ridging and clubbing. [23]
Central nervous system
Destruction of tips of digits is seen in Lesch-Nyhan syndrome. Onychomadesis is noted in peripheral neuritis and hemiplegia. Beau′s lines are reported in patients with epilepsy. [1]
Nail changes in psychological disorders
Abnormalities of the nail unit may occur in association with several psychological and psychiatric illnesses. A significant correlation exists between family history of schizophrenia and visibility of the subcapillary plexus in the nail fold. Striated leukonychia is noted in manic-depressive illness. [1] Onychotillomania, an extreme form of self mutilation of the nails is thought to be an obsessive-compulsive disorder. [1]
Autoimmune disorders [24]
- Systemic lupus erythematosus (SLE): Erythema of proximal nailfold, splinter hemorrhages, capillary loops in proximal nail fold, thin nail-plate, ragged cuticle and periungual erythema in fingernails are common. Beau′s line, periungual telengiectasia and capillary loops are also reported.
- Systemic sclerosis (SSc): Capillary loops in proximal nailfold, splinter hemorrhages, longitudinal and transverse curvature in fingernails digital pitted scars are frequent.
- Rheumatoid arthritis: Splinter hemorrhages, red lunula and white dull colour in fingernails are common.
- Dermatomyositis and polymyositis: Splinter hemorrhages, capillary loops in proximal nailfold in fingernails, periungual erythema, periungual telangiectasia and capillary loops in proximal nailfold have been reported.
IV. Nail Abnormalities Associated with Specific Syndromes or Genodermatoses
- Darier′s disease - longitudinal streaks, "V" shaped notch. [1]
- Dyskeratosis congenita - koilonychia, onychorrhexis, onychoschizia. [1]
- Pachyonychia congenita - subungual hyperkeratosis. [1]
- Nail - patella syndrome - triangular lunulae. [1]
- Incontinentia pigment - periungual / subungual tumors. [1]
- Reiter′s syndrome - subungual hyperkeratosis, onycholysis, and brownish discolouration, pitting. [25]
- Trichothiodystrophy - brittle nails. [25]
Diagnosis
Diagnosis of nail changes in systemic diseases is essentially clinical.
- Mycology: Potassium hydroxide (KOH) wet mount to exclude onychomycosis.
- Biopsy: fungal cultures may be required to confirm onychomycosis.
- Nailfold capillaroscopy: is useful for evaluation of nail changes in collagen disorders. Nail fold capillaries provide a readily available window to view the microvascular pathology of collagen vascular disease. Nail fold capillaroscopy is the oldest and arguably the best technique for investigating microvascular involvement in rheumatic disease. The dermatoscope is the preferable capillaroscopic instrument as it has a larger field of view than that of an ophthalmoscope. [26]
- Radiology: Technetium Tc 99m skeletal imaging may be helpful in determining the presence and extent of bone changes in clubbed digits, which show increased uptake of the radionuclide.
- Thermography and positron emission tomography. [27],[28] These are few imaging studies used for diagnosis and monitoring of nails in systemic diseases.
Acknowledgement
Author gratefully acknowledges the assistance by Dr. Lavanya MS, and Dr. Nayeem Sadath Haneef in preparation of manuscript.
| 1. |
Lawry M, Daniel CR 3 rd . Nails in systemic disease. In: Scher RK, Daniel CR, editors. Nails: Diagnosis, Therapy, Surgery. 3 rd ed. Philadelphia: Elsevier Science Limited; 2005. p. 147-69.
[Google Scholar]
|
| 2. |
Monk BE. The prevalence of splinter haemorrhages. Br J Dermatol 1980;103:183-5.
[Google Scholar]
|
| 3. |
Daniel CR, Sams WM, Scher RK. Nails in systemic disease. Dermatol Clin 1985;3:167-87.
[Google Scholar]
|
| 4. |
De Barber D. What do Beau's lines mean. Int J Dermatol 1996;134:542-7.
[Google Scholar]
|
| 5. |
Weissman K. J H S Beau and his descriptions of transverse depressions on nails. Br J Dermatol 1977;97:571-2.
[Google Scholar]
|
| 6. |
Meyerson MS, Scher RK. Nail signs of systemic disease. In: Callen JP, Jorizzo JL, Greer KE, Penneys NS, Piette WW, Zone JJ, editors. Dermatological signs of internal disease. 2 nd ed. Philadelphia: WB Saunders Co.; 1999. p. 368-75.
[Google Scholar]
|
| 7. |
Ray L. Onycholysis: A classification and study. Arch Detmatol 1963;88:181-5.
[Google Scholar]
|
| 8. |
Jadhav VM, Mahajan PM, Mhaske CB. Nail pitting and onycholysis. Indian J Dermatol Venereol Leprol 2009;75:631-3.
[Google Scholar]
|
| 9. |
Kechijian P. Onycholysis of the fingernails: Evaluation and management. J Am Acad Dermatol 1985;12:552-60.
[Google Scholar]
|
| 10. |
Tosti A, Daniel CR, Piccorini BM, Iorizzo M. Color Atlas of Nails. Heidelberg: Springer Verlag; 2010. p. 3
[Google Scholar]
|
| 11. |
Zaiac MN, Daniel CR. Nails in systemic disease. Dermatol Ther 2002;5:99-106.
[Google Scholar]
|
| 12. |
Grossman M, Scher RK. Leukonychia: Review and classification. Int J Dermatol 1990;29:535-41.
[Google Scholar]
|
| 13. |
Marino MJ. Mee's lines. Arch Dermatol 1990;126:827-8.
[Google Scholar]
|
| 14. |
Gregoriou S, Argyriou G, Larios G, Rigopoulos D. Nail disorders and systemic disease: What the nails tell us. J Fam Pract 2008;57:509-14.
[Google Scholar]
|
| 15. |
Goodman GJ, Nicolopoulos J, Howard A. Diseases of the generative nail apparatus. Part II: Nail bed. Australas J Dermatol 2002;43:157-70.
[Google Scholar]
|
| 16. |
Fawcett RS, Linford S, Stulberg D. Nail abnormalities: Clues to systemic disease. Am Fam Physician 2004;69:1417-24.
[Google Scholar]
|
| 17. |
Saray Y, Seckin D, Gulec AT, Akgun S, Haberal M. Nail disorders in hemodialysis patients and renal transplant recipients: A case-control study. J Am Acad Dermatol 2004;50:197-202.
[Google Scholar]
|
| 18. |
Shearn MA. Nails and systemic disease. West J Med 1978;129:358-63.
[Google Scholar]
|
| 19. |
Moffitt, De Berker R. Yellow nail syndrome: The nail that grows half as fast grows twice as thick. Clin Exp Dermatol 2000;25:21-3.
[Google Scholar]
|
| 20. |
dos Santos VM, Marques HV Jr, Lima Cdo C, Turra TZ, de Melo Nogueira PR Jr, Lima LN. Yellow nail syndrome and adnexal tumour: Causal or casual association? Indian J Chest Dis Allied Sci 2010;52:51-3.
[Google Scholar]
|
| 21. |
Salem A, Gamil H, Hamed M, Galal S. Nail changes in patients with liver disease. J Eur Acad Dermatol Venereol 2010;24:649-54.
[Google Scholar]
|
| 22. |
Rich P. Nail changes due to diabetes and other endocrinopathies. Dermatol Ther 2002;15:107-10.
[Google Scholar]
|
| 23. |
Cribier B, Leiva-Mena M, Rey D, Partisani M, Fabien V, Marie-Lang J. Nail changes in patients infected with human immunodeficiency virus. Arch Dermatol 1998;134:1216-20.
[Google Scholar]
|
| 24. |
Tunc S, Ertam I, Pirildar T, Turk T, Ozturk M, Doganavsargil E. Nail changes in connective tissue diseases: Do nail changes provide clues for the diagnosis? J Eur Acad Dermatol Venereol 2007;21:497-503.
[Google Scholar]
|
| 25. |
Rich P, Scher RK. An atlas of diseases of the nail. New York: Parthenon Publishing; 2003.
[Google Scholar]
|
| 26. |
Sherber NS, Wigley FM, Scher RK. Autoimmune disorders: Nail signs and therapeutic approaches. Dermatol Ther 2007;20:17-30.
[Google Scholar]
|
| 27. |
Rush PJ, Giorshev C, Shore A, Levinson H. The use of thermography in clubbing. Respir Med 1992;86:257-9.
[Google Scholar]
|
| 28. |
Ward RW, Chin R, Keyes JW, Haponik EF. Digital clubbing. Demonstration with positron emission tomography. Chest 1995;107:1172-3.
[Google Scholar]
|
Fulltext Views
23,353
PDF downloads
6,376





![[Figure - 1]](#fig_ijdvl_2011_77_6_646_86472_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2011_77_6_646_86472_f2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2011_77_6_646_86472_f3.jpg){kind=link}