Translate this page into:
Neurofollicular hamartoma
2 Department of Dermatology, Goztepe Training and Research Hospital, Istanbul Medeniyet University, Istanbul, Turkey
Correspondence Address:
Seyma Ozkanli
Tutuncu Mehmet Efendi Cad., Karanfil Sok., Ugur Apt. No: 16/3, Goztepe, Istanbul
Turkey
| How to cite this article: Zemheri E, Engin P, Ozkanli S, Zindanci I, Zenginkinet T, Karadag AS. Neurofollicular hamartoma. Indian J Dermatol Venereol Leprol 2016;82:329-330 |
Sir,
Formerly, follicular neoplasms composed of epithelial and stromal components have been described as angiofibroma, fibrofolliculoma, trichogenic myxoma and trichodiscoma. Barr and Goodman in 1989 described a new entity which did not fit in with any previously recognized follicular neoplasms and named it neurofollicular hamartoma.[1]
A 63-year-old male presented with a tan colored papule on his nose [Figure - 1]. With a diagnosis of intradermal nevus, the lesion was excised. Histopathological examination revealed a well-defined unencapsulated lesion in the dermis composed of an epithelial component with hyperplastic sebaceous glands, distorted hair follicles and a stromal component with spindle-shaped cells and dendritic cells arranged in short fascicles or haphazardly in a myxoid stroma [Figure - 2]. This stroma was positive with PAS-Alcian Blue staining. The spindle cells stained positively with S-100 [Figure - 3] and neuron specific enolase and did not stain with CD34. In addition, the peritumoral stroma and spindle cells were stained with S-100. With these results, the case was diagnosed as neurofollicular hamartoma.
 |
| Figure 1: Tan colored papule on the nose |
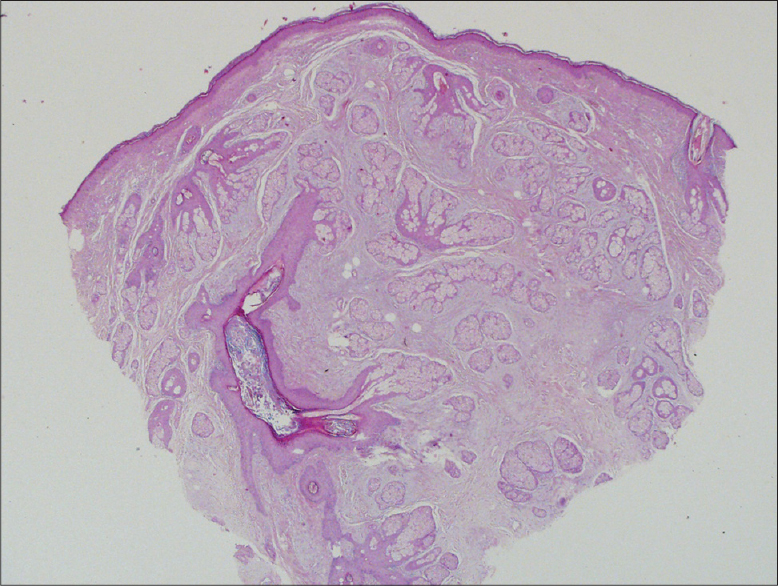 |
| Figure 2: Well-defined unencapsulated lesion composed of hyperplastic sebaceous glands, distorted hair follicles and spindle cells. (H and E, 40×4) |
 |
| Figure 3: Spindled and dendritic cells stained with S-100 antibody (×100) |
Neurofollicular hamartoma is a rare and relatively newly described neoplasm. It is a distinct entity showing a distorted hyperplastic pilosebaceous unit and a stromal component consisting of elongated spindle cells arranged in fascicles, short bundles or haphazardly in a myxoid stroma. Pilosebaceous units may show basaloid, sebaceous, squamous or ductal epithelial proliferation.[1]
Immunohistochemically, spindle and dendritic cells stain positively with S-100 protein and neuron specific enolase.[1],[2] Although earlier reported cases of neurofollicular hamartoma have described positive staining of spindle cells with CD34, in recent textbooks, neurofollicular hamartoma is known as a S-100 positive and CD34 negative proliferation.[2] The neurofollicular hamartoma has bcl-2 staining of basaloid nests and cords. The peritumoral stroma of neurofollicular hamartoma and matricial cells also exhibit CD10 staining.[3] In our case, spindle cells stained positive with S-100 and neuron specific enolase and were CD 34 negative. Neurofollicular hamartoma usually presents as a single, asymptomatic, 2-7 mm skin-colored papule located on the face, usually near the nose.[1] The age of presentation ranges from 37 to 72 years with a mean of 60 years.[1] It clinically resembles fibrous papule, intradermal nevus or basal cell carcinoma.
It should be differentiated from other tumors with prominent perifollicular mesenchyme including fibrofolliculoma and trichodiscoma. The fibrofolliculoma is an infundibulocentric tumor that consists of anastomotic strands and cords without fully formed follicles. Sebocytes may be seen within the epithelial cords. Around the epithelial cords, there is a well-circumscribed proliferation of loose connective tissue with mucin. The trichodiscoma is a well-demarcated tumor that is composed of fascicles of loose, finely fibrillary connective tissue with abundant mucin. At the periphery of the connective tissue, fibrofolliculoma-like areas may be seen. The stromal cells in both lesions are CD34 positive and negative for S-100, smooth muscle actin, epithelial membrane antigen and desmin.[2],[4] Fibrofolliculomas and trichodiscomas have a different histopathology but they have been reported to exist synchronously in Birt–Hogg–Dube syndrome associated with multiple fibrofolliculomas, trichodiscomas and acrochordons.[5]
According to Sangueza and Requena, neurofollicular hamartomas, trichodiscomas and fibrofolliculomas lie in the same hamartomatous spectrum. Fibrofolliculoma and trichodiscoma lie at extreme ends of the spectrum while neurofollicular hamartoma lies in the middle of the spectrum.[5]
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
| 1. |
Barr RJ, Goodman MM. Neurofollicular hamartoma: A light microscopic and immunohistochemical study. J Cutan Pathol 1989;16:336-41.
[Google Scholar]
|
| 2. |
Calorje E, Lazac A, Mckee PH. Mckee's Pathology of the Skin. 4th ed., Vol. 2. China: Elsevier Sounders; 2012. p. 1486-7.
[Google Scholar]
|
| 3. |
Ramos-Ceballos FI, Pashaei S, Kincannon JM, Morgan MB, Smoller BR. Bcl-2, CD34 and CD10 expression in basaloid follicular hamartoma, vellus hair hamartoma and neurofollicular hamartoma demonstrate full follicular differentiation. J Cutan Pathol 2008;35:477-83.
[Google Scholar]
|
| 4. |
Kutzner H, Requena L, Rütten A, Mentzel T. Spindle cell predominant trichodiscoma: A fibrofolliculoma/trichodiscoma variant considered formerly to be a neurofollicular hamartoma: A clinicopathological and immunohistochemical analysis of 17 cases. Am J Dermatopathol 2006;28:1-8.
[Google Scholar]
|
| 5. |
Sidhu HK, Patel RV, Goldenberg G. Dermatology clinics: What's new in dermatopathology: News in nonmelanocytic neoplasia. Dermatol Clin 2012;30:623-41, vi.
[Google Scholar]
|
Fulltext Views
4,097
PDF downloads
3,232





![[Figure - 1]](#fig_ijdvl_2016_82_3_329_175921_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2016_82_3_329_175921_f2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2016_82_3_329_175921_f3.jpg){kind=link}