Translate this page into:
Nevoid hyperkeratosis of nipple: Nevoid or hormonal?
Correspondence Address:
Siddhi B Chikhalkar
Department of Dermatology, Seth GSMC and KEM Hospital, Parel, Mumbai - 400 012
India
| How to cite this article: Chikhalkar SB, Misri R, Kharkar V. Nevoid hyperkeratosis of nipple: Nevoid or hormonal?. Indian J Dermatol Venereol Leprol 2006;72:384-386 |
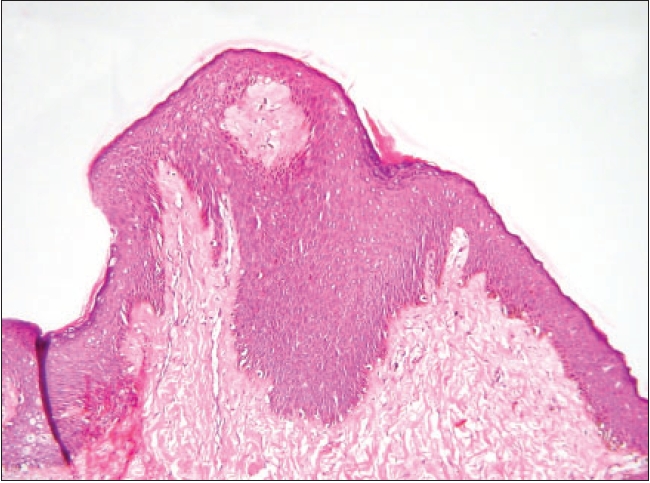 |
| Papillomatosis and acanthosis (H and E, 200x) |
|
| Papillomatosis and acanthosis (H and E, 200x) |
 |
| Pretreatment (a) and post-treatment (b) photographs of palms and soles |
|
| Pretreatment (a) and post-treatment (b) photographs of palms and soles |
Sir,
We read with the interest the article "Nevoid hyperkeratosis of nipple - a report of two cases" in your journal recently.[1] We hereby report a case of nevoid hyperkeratosis of nipple and areola (HNA). We were intrigued by the term ′Nevoid′ and hence try to debate as to how appropriate is the use of this terminology. Also, till date only two cases of nevoid hyperkeratosis of nipple have been reported from India.[1],[2]
A 21-year-old female presented to us with asymptomatic brown-colored rough raised lesions on both the nipples since the age of 13 years. The lesions increased in size during pregnancy. There was no history of pruritus, alteration in the lesion with menstrual cycle and complications such as ulceration, bleeding, discharge, pain or retraction of nipple. There was no history of any other skin lesions at that site.
On examination both the nipples were covered with diffuse, hyperpigmented, verrucous and hyperkeratotic plaque [Figure - 1]. No associated anomalies of the nipples and breast were seen. The skin biopsy of the lesion showed irregular acanthosis and papillomatosis with increased melanization of keratinocytes. Melanocytes were normal in number [Figure - 2]. Based on clinical and histopathological features we reached the diagnosis of nevoid hyperkeratosis of the nipple. Since the patient was pregnant (five months gravida) we counseled her and advised follow-up after delivery for treatment.
HNA is a rare clinical condition. Initially described in 1923,[2] HNA is classified into three categories according to the classification proposed by Levy-Frenckel in 1938:[3],[4] Type I: associated with an epidermal nevus, Type II: associated with other dermatoses (congenital, acquired or erythrodermic ichthyosis, acanthosis nigricans, Darier′s disease, chronic eczema, cutaneous T-cell lymphoma) and Type III: (Nevoid HNA), of unknown etiology, an isolated finding.
Considering the above classification, our patient had Type III HNA. Amongst the various types, nevoid form of the disease is extremely rare, usually seen in women in the second or third decade of life. There are doubts on whether nevoid hyperkeratosis of the nipple and areola is a distinct entity or a clinical presentation of various dermatoses. Type III HNA is seen in females at puberty, those of childbearing age, pregnancy and also in males receiving hormonal therapy for prostate cancer.[5],[6] It may also be seen in females and males without the above mentioned conditions. Pregnancy may increase the size of the lesions. Since our patient′s condition began at puberty and worsened during pregnancy the term hormonal hyperkeratosis of nipple would be more apt.
Even Mehanna et al .[7] suggested that Type I should not be considered as HNA as it is associated with the epidermal nevus and hence the term should be reserved for only Types II and III. They also suggested that the term ′nevoid′ be replaced by ′idiopathic′. The term nevoid[8] (nevus-like) means odd or abnormal that stems from a heritable or embryogenic fault. So one really wonders whether the term nevoid is truly applicable here and hence revision of the term has to be considered. Hence we support the view of Mehanna et al. that the term nevoid should not be used for the Type III variant of HNA.
Perez-Izquierdo et al .[9] proposed an alternative classification of two types:
1. Idiopathic or nevoid
2. Secondary to other dermatoses.
The main cause of concern for patients of HNA is the cosmetic appearance of the nipple and areola. Patients should be asked to look out for any changes in the breasts. They should be counseled about the condition and the treatment that may take a long time. Treatment with one of the medications as mentioned by Veeranna et al .[1] should be continued for at least six months before it is considered a failure. Sometimes lesions recur and in some patients lesions don′t respond to treatment.[3] Since our patient was pregnant, counseling was done and we asked the patient to follow up for treatment after delivery.
| 1. |
Veeranna S, Betkerur J, Kushalappa PA. Unilateral nevoid hyperkeratosis of the nipple: A report of two cases. Indian J Dermatol Venereol Leprol 2006;72:303-5.
[Google Scholar]
|
| 2. |
Baykal C, Buyukbabani N, Kavak A, Alper M. Nevoid hyperkeratosis of the nipple and areola: A distinct entity. J Am Acad Dermatol 2002;46:414-8.
[Google Scholar]
|
| 3. |
Revert A, Banuls J, Montesinos E, Jorda E, Ramon D, Torres V. Nevoid hyperkeratosis of the areola. Int J Dermatol 1993;32: 745-6.
[Google Scholar]
|
| 4. |
Burns DA. The Breast, In: Tony Burns, Breathnach S, Cox N, Griffith C, editors. Rook's Textbook of Dermatology, 7th ed. Blackwell Science: New York; 2004. p. 67.8-9.
[Google Scholar]
|
| 5. |
Kubota Y, Koga T, Nakayama J, Kiryu H. Naevoid hyperkeratosis of the nipple and areola in a man. Br J Dermatol 2000;142: 382-4.
[Google Scholar]
|
| 6. |
English JC 3rd, Coots NV. A man with nevoid hyperkeratosis of the areola. Cutis 1996;57:354-6.
[Google Scholar]
|
| 7. |
Mehanna A, Malak JA, Kibbi AG. Hyperkeratosis of the nipple and areola: Report of 3 cases. Arch Dermatol 2001;137:1327-8.
[Google Scholar]
|
| 8. |
Leider M, Rosenblum M. A dictionary of dermatological words, Terms and phrases. McGraw Hill Book Company: New York; 1968. p. 297.
[Google Scholar]
|
| 9. |
Perez-Izquierdo J, Vilata J, Sanchez J, Gargallo E, Millan F, Aliaga A. Retinoic treatment of nipple hyperkeratosis. Arch Dermatol 1990;126:687-8.
[Google Scholar]
|
Fulltext Views
3,613
PDF downloads
777





![[Figure - 1]](#fig_ijdvl_2006_72_5_384_27762_1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2006_72_5_384_27762_2.jpg){kind=link}