Translate this page into:
Onychomatricoma: An infrequent nail tumor
2 Department of Pathology, Instituto Nacional de Ciencias M�dicas y Nutrici�n Salvador Zubir�n, M�xico City, Mexico
Correspondence Address:
M�nica Fern�ndez-S�nchez
Centro M�dico ABC Santa Fe, Av. Carlos Graef Fern�ndez 154 Consultorio 307, Torre de Consultorios, Col Tlaxala Santa Fe, CP 05300, Mexico City
Mexico
| How to cite this article: Fern�ndez-S�nchez M, Saeb-Lima M, Charli-Joseph Y, M�ndez-Flores S, S�nchez-Hern�ndez C, Carbajosa-Martinez J. Onychomatricoma: An infrequent nail tumor. Indian J Dermatol Venereol Leprol 2012;78:382-383 |
Sir,
Onychomatricoma is a rare subungual tumor of unknown etiology that affects the nail apparatus. It consists of a thickened yellowish nail with transverse over-curvature, ridging and dystrophy. Additionally, there may be longitudinal melanonychia, proximal nail swelling and splinter hemorrhages found in capillaroscopy. We herein, describe two Mexican patients with onychomatricoma.
Patient #1 is a 59-year-old woman with a 20-year history of nail deformity affecting the second left finger, characterized by painful central linear subungual hyperkeratosis and onycholysis [Figure - 1]a. She denied any trauma or bleeding and the rest of the finger and toe-nails were normal. A diagnosis of subungual fibroma was suggested and excision of the nail matrix performed. The biopsy [Figure - 1]b showed an epithelial tumor, affecting the nail plate and matrix composed of fibrous stroma, in which digitated strands of small basaloid cells with round nuclei and scant cytoplasm were embedded. In some areas, a thick keratinous zone was seen over such strands and occasionally calcium deposits were observed. By immunohistochemistry, tumor cells stained positive for cytokeratin 5, 6 and pankeratin. After clinicopathological correlation, a definitive diagnosis of onychomatricoma was established.
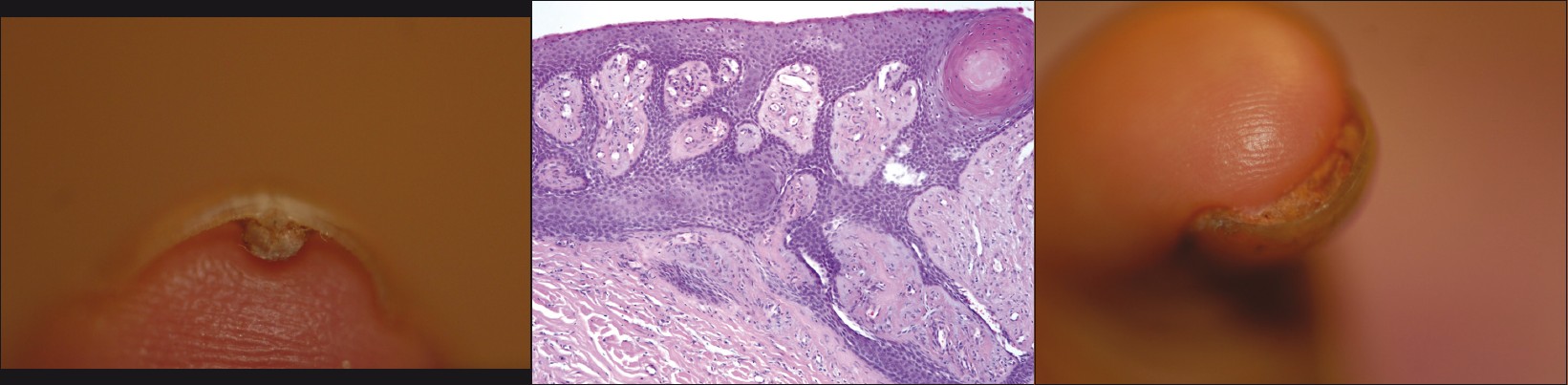 |
| Figure 1a: Subungual view of the nail showing a central and well-delimited hyperkeratotic tumor Figure 1b: Fibroepithelial tumor composed of strands of small basaloid cells with round nuclei and scant cytoplasm; the stroma is fibroblastic with increased vascularization (H and E, ×40) Figure 1c: A subungual tumor (onychomatricoma) presenting as hyperkeratosis and paronychia |
Patient #2 is a 38-year-old woman with diabetes mellitus and tuberous sclerosis who presented with a 3-year history of multiple nail deformities characterized by subungual and periungual tumors (Koenen tumors), as well as onychomadesis and paronychia of the first left fingernail [Figure - 1]c, previously treated unsuccessfully as onychomycosis albeit a negative fungal culture. A diagnosis of subungual fibroma was suggested and a nail biopsy demonstrated fibroepithelial tumor of the matrix and nail plate composed of fibrous stroma with digitations of small basaloid cells and occasional calcium deposition; pankeratin and cytokeratin 5-6 immunohistochemistry was positive. The possibility of a Koenen tumor was ruled out and an onychomatricoma was finally diagnosed.
Baran and Kint first described onychomatricoma and confirmed the nail matrix origin of the tumor. [1] However, other authors have proposed it as a fibroproliferative hamartoma that simulates the nail matrix histology. [2] Onychomatricoma has a female to male ratio of 2.16:1; mean age of presentation is 51 years and occurs more frequently in Caucasian patients. Less frequently, it occurs in African Americans and exceptionally in Mexican patients. Its predominant location is the fingernails (75%). Predisposing factors such as trauma or onychomycosis have been suggested.
Pathology shows a wide histological spectrum as recently described by Perrin et al., [3] but typically consists of fibroepithelial tumor composed of a proximal pedunculated base and a distal zone with multiple projections. There is a two-layered stroma with a collagenous and fibroblastic superficial coat and a deep core with less cellularity and thicker collagen; a V-shaped hyperkeratogenous zone can be observed. Beyond the lunula, the nail plate is thickened and burrowed with cavities containing serous fluid. Immunohistochemistry for cytokeratin 5 and 14 are positive, along with K17, K6, K16, and K75 in most cases, suggesting a differentiation towards the nail bed and the nail isthmus. [4] Recently CD34 was also reported to be positively expressed. [3]
Magnetic resonance shows tumoral core in the matrix with invaginations into the funnel-shaped nail plate; the center has a low intensity signal and peripheral and axial images show the holes in the nail plate and the tumoral digitations. [5]
Differential diagnosis for onychomatricoma include fibrokeratoma of the nail matrix, glomus tumor, squamous cell carcinoma, Bowen′s disease, viral warts and ungual fibroma. This last diagnosis was the clinical impression in both patients described above; however, it can be ruled out by the hyperplastic and onychogenic nature of the epithelium. Complete surgical excision is the first line of treatment. Recurrence and malignant transformation have not been reported, although dysplasia may be present. [3]
Onychomatricoma is an infrequent subungual tumor that primarily occurs in Caucasians. Only two cases have been previously reported in Mexican patients. Treatment should be individualized but complete surgical excision remains as the gold standard. Because onychomatricoma can easily mimic other ungual diseases, physicians and particularly dermatologists should be acquainted with the proper diagnosis and treatment of this adnexal tumor.
| 1. |
Baran R, Kint A. Onychomatrixoma. Filamentous tufted tumor in the matrix of a funnel-shaped nail: A new entity (report of three cases). Br J Dermatol 1992;126:510-5.
[Google Scholar]
|
| 2. |
Kint A, Baran R, Geerts ML. The onychomatricoma: An electron microscopic study. J Cutan Pathol 1997;24:183-8.
[Google Scholar]
|
| 3. |
Perrin C, Baran R, Balaguer T, Chignon-Sicard B, Cannata GE, Petrella T, et al. Onychomatricoma: New clinical and histological features. A review of 19 tumors. Am J Dermatopathol 2010;32:1-8.
[Google Scholar]
|
| 4. |
Perrin C, Baran R, Pisani A, Ortonne JP, Michiels JF. The onychomatricoma: Additional histologic criteria and immunohistochemical study. Am J Dermatopathol 2002;24:199-203.
[Google Scholar]
|
| 5. |
Goettmann S, Drape JL, Baran R, Perhn C, Haneke E, Belaich S. Onychomatricome: Deuxnouveauxcas. Interet de la resonance magnetiquenucleaire. Ann DermVenereol 1994;121: S145.
[Google Scholar]
|
Fulltext Views
5,410
PDF downloads
2,355





![[Figure - 1]](#fig_ijdvl_2012_78_3_382_95459_f1.jpg){kind=link}