
Translate this page into:
Painful, extensive, yellowish nodules on fingers
Corresponding author: Dr. Yoon-Seob Kim, Department of Dermatology, The Catholic University of Korea, Seoul, Republic of Korea. kysbbubbu@catholic.ac.kr
-
Received: ,
Accepted: ,
How to cite this article: Ju S, Kim Y-S. Painful, extensive, yellowish nodules on fingers. Indian J Dermatol Venereol Leprol. doi: 10.25259/IJDVL_1681_2024
A 67-year-old man presented with multiple, painful, yellowish
nodules which had persisted for two years [Figures 1a and 1b]. He had no other notable medical history or systemic symptoms. Histopathological examination showed nodular deposits of amorphous, crystalline, pink material surrounded by chronic granulomatous inflammation and multinucleated foreign body giant cells throughout the dermis [Figures 2a and 2b]. The laboratory tests showed elevated levels of C-reactive protein (20.31 mg/L; normal range 0–5 mg/L), blood urea nitrogen (29.1 mg/dL; normal range 6.0–20.0 mg/dL), creatinine (1.76 mg/dL; normal range 0.7–1.2 mg/dL), and uric acid (11.2 mg/dL; normal range 3.4–7.0 mg/dL). The estimated glomerular filtration rate was lowered (39 mL/min/1.73 m2; normal range >59 mL/min/1.73 m2). There were no abnormalities in lipid, calcium, or phosphate levels.
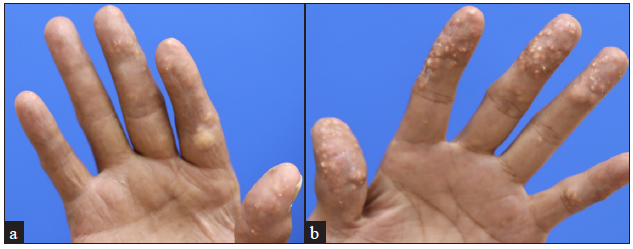
- Extensive yellowish nodules involving palmer aspect of fingers of both hands.
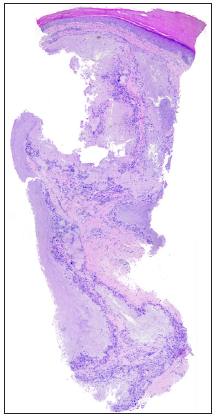
- Nodular deposits of amorphous pink material in the dermis surrounded by chronic granulomatous inflammation (Haematoxylin & eosin, 20x).
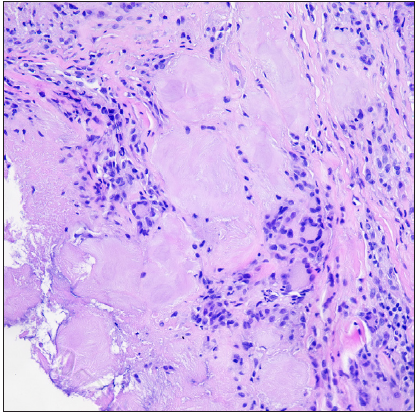
- Nodular deposits of amorphous pink material in the dermis surrounded by chronic granulomatous inflammation with multinucleated foreign body giant cells (Haematoxylin & eosin, 200x).
Question
What is your diagnosis?
Answer
Diagnosis: Tophaceous gout.
Discussion
Gout is a metabolic disorder characterised by acute or chronic arthritis resulting from the deposition of monosodium urate crystals in joints, bones and other tissues.1 Tophaceous gout refers to the chronic deposition of monosodium urate crystals in the skin and soft tissues. It is typically a prolonged and poorly managed disease.2,3 Tophaceous gout commonly presents as yellowish nodules with granulomatous inflammation within the dermal and subcutaneous tissues. It often occurs near joints, tendons or other areas such as the helix and finger pads.3 Less common cutaneous manifestations include papules, ulcers and pustules.4 Tophi usually appear approximately 12 years after the first gout attack and can cause pain, tissue damage, joint deformities and nerve compression.1
Direct extraction of material from a skin lesion can reveal the characteristic elongated crystals with birefringence under polarised light to confirm the diagnosis.3 Alternatively, routine biopsy with formalin fixation, as in this case, may reveal amorphous deposits encircled by a granulomatous inflammation, which is sufficient for the diagnosis.3
Differential pathological diagnoses for amorphous pink deposits in the dermis include calcinosis cutis, pseudogout and amyloidosis. Calcinosis cutis typically shows basophilic calcium deposits on haematoxylin and eosin (H&E) staining; they also stain positively with von Kossa stain.3 Pseudogout, also known as calcium pyrophosphate dihydrate crystal deposition disease (CPPD), presents as faintly eosinophilic crystals that are smaller and less birefringent under polarised light compared with the monosodium urate crystals found in gout.5 Amyloidosis is distinguished by amorphous eosinophilic material that stains positively with Congo red and demonstrates apple-green birefringence under polarised light.
Clinical differential diagnoses for finger nodules include tuberous xanthoma, knuckle pads and granuloma annulare. Tuberous xanthomas are associated with hyperlipidaemia and present as firm, yellowish nodules on extensor surfaces. The histology shows collections of lipid-laden macrophages without crystalline deposits.3 Knuckle pads appear as firm, flesh-coloured plaques over the dorsal aspects of interphalangeal joints and are devoid of significant histological findings. Granuloma annulare typically manifests as annular plaques, particularly on the extremities and histologically shows palisading granulomas surrounding necrobiotic collagen.3
Treatment of tophaceous gout involves dietary modification and pharmacologic management to lower uric acid levels using xanthine oxidase inhibitors (e.g., allopurinol, febuxostat) or uricosuric agents (e.g. probenecid). Acute attacks are managed with colchicine and nonsteroidal anti-inflammatory drugs, while surgical excision is reserved for significant joint deformities, intractable pain, or chronic ulceration.1
In this case, the patient was referred to a rheumatologist, who confirmed the diagnosis and initiated treatment with febuxostat (80 mg daily), colchicine (0.3 mg daily), and prednisolone (5 mg daily), resulting in rapid pain relief. His mild renal impairment may have contributed to the onset of tophaceous gout. This case highlights the importance of considering tophaceous gout in patients presenting with atypical papules or nodules on the fingers, ears, or soles, even without a prior history of gout. Early diagnosis can facilitate timely urate-lowering therapy, potentially limiting future gout attacks and systemic complications.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
References
- Multiple asymptomatic juxta-articular nodules mimicking tuberous-xanthoma-A unusual presentation of tophaceous gout. J Cutan Aesthet Surg. 2017;10:223-5.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Atypical cutaneous presentation of chronic tophaceous gout: A case report. Indian Dermatol Online J. 2020;11:235-8.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- From skin to microscope, case report of a rare manifestation of tophaceous gout: Miliary gout. Int J Rheum Dis. 2024;27:e14763.
- [CrossRef] [PubMed] [Google Scholar]
- Multiple cutaneous creamy papules and nodules: A case of miliarial gout. J Cutan Med Surg. 2015;19:317-9.
- [CrossRef] [PubMed] [Google Scholar]
- Calcium pyrophosphate deposition disease. N Engl J Med. 2016;374:2575-84.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]




