Translate this page into:
Painless dells on the cheek
2 Department of Pathology, Acıbadem University School of Medicine, Istanbul, Turkey
3 Department of Plastic, Reconstructive and Aesthetic Surgery, Acıbadem University School of Medicine, Istanbul, Turkey
Correspondence Address:
Emel �zt�rk Durmaz
Acıbadem Maslak Hospital, B�y�kdere Caddesi 40, Maslak 34457, Istanbul
Turkey
| How to cite this article: Duman D, Durmaz E�, �etin ED, Yazar &, Şahin S. Painless dells on the cheek. Indian J Dermatol Venereol Leprol 2013;79:847-848 |
A 30-year-old woman presented with a 15-year history of two asymptomatic dells on her right cheek. There was no history of preceding acne or inflammatory skin disease.
Dermatologic examination revealed two 0.5 cm and 0.3 cm-sized, sharply-demarcated, skin-colored papules with cup-shaped central depressions, located on the zygomatic [Figure - 1] and mandibular regions of the right cheek. On close inspection, follicular plugging was evident.
 |
| Figure 1: A well-circumscribed umbilicated patch on the right zygomatic region |
Histopathological examination displayed a partially well-circumscribed tumor in the dermis with an overlying sharp depression. The tumor was composed of small cords and islands of basaloid cells that showed connection to the follicular infundibulum. Tumor strands were surrounded by a desmoplastic fibrous stroma [Figure - 2] and [Figure - 3]. Several keratinous cysts and foci of dystrophic calcification were also noted. Immunohistochemically, the tumor cells stained positive with anti-pancytokeratin (CK), anti-CK15 and negative with anti-carcinoembryonic antigen (CEA), anti-CK7 and anti-epithelial membrane antigen antibodies. The tumor was focally immunopositive for CK20 antibody, indicating the presence of scattered Merkel cells.
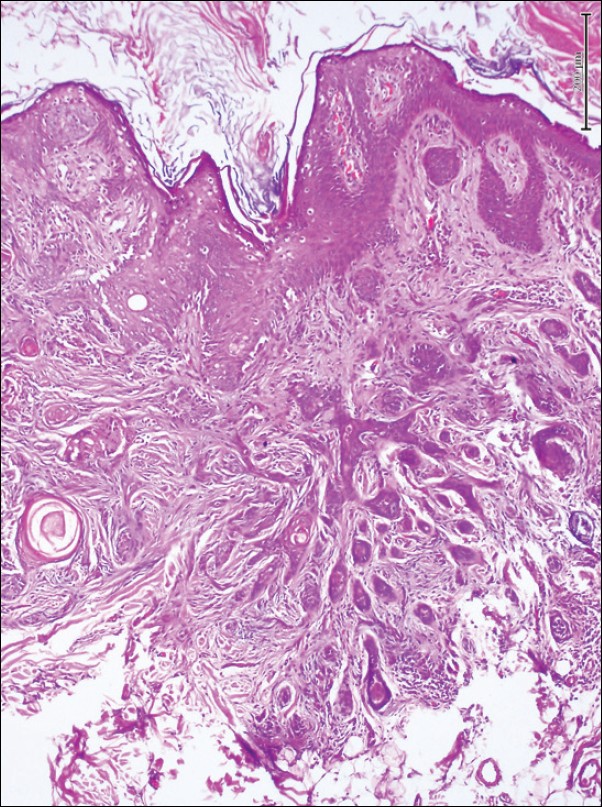 |
| Figure 2: Thin cords and islands of basaloid cells in a dense fibrous stroma (H and E, ×100) |
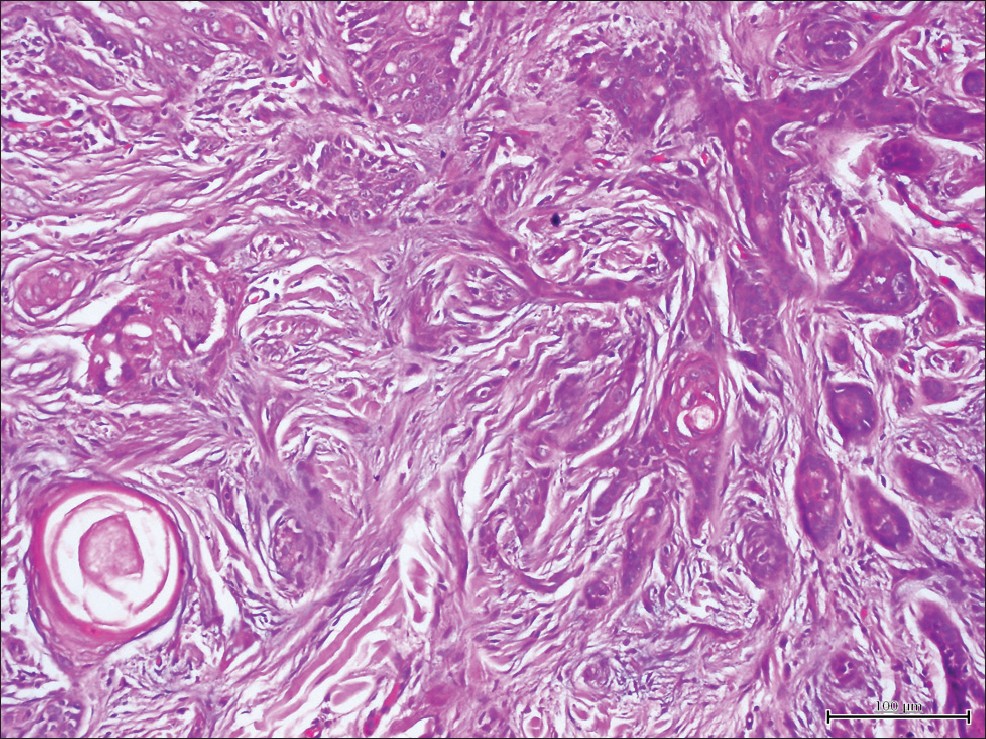 |
| Figure 3: Closer view of Figure 2 (H and E, ×200) |
What is Your Diagnosis?
Discussion
Desmoplastic trichoepithelioma (DTE) is a rarely encountered benign adnexal tumor with an estimated incidence of 2 in 10.000 skin biopsies. [1],[2] The age range varies from 0 to 80. The lesion usually develops on the face of a young woman (71-85%). [2] The cheek is the most frequent site of affection (50%). [1],[2],[3] There is a propensity for DTE development on the right side of the face. [2] DTE presents as an asymptomatic, solitary, annular, firm, white to yellowish papule or as a sclerotic plaque smaller than 2 cm. The lesion has a thread-like raised and rolled border and a non-ulcerated central dell. [1],[2] The clinical appearance may be reminiscent of basal cell carcinoma (BCC).
The histologic portrait in previous reports encompasses narrow strands of basaloid cells, keratinous cysts and desmoplastic stroma. [2] The well-demarcated solid tumor is situated symmetrically within the papillary and reticular dermis. [2],[3] Small basaloid cells with prominent oval nuclei and scant cytoplasm are arranged in slender strands containing one to three rows of cells. There is often a focal connection to the overlying epidermis through the follicular infundibulum. The stroma surrounding the strands of basaloid cells consists of ample homogeneous eosinophilic collagen and multiple horn cysts. There is no cleft between the nests of tumor cells and sclerotic stroma. While palisading is lacking, epidermal hyperplasia may be noted. [2] Foreign body granulomas from broken cysts, areas of calcification or ossification might be observed. [2],[4]
The list of differential diagnostic considerations embraces trichoadenoma, trichoepithelioma, syringoma, sebaceous hyperplasia, granuloma annulare, BCC, microcystic adnexal carcinoma and squamous cell carcinoma. [2] Differentiation from morphea-like BCC may be extremely difficult, especially when a lesion is sampled only in part. Immunohistochemical markers may help the pathologist to distinguish DTE and morphea-like BCC. In particular, identification of CK20-positive Merkel cells within the lesion, the presence of CK15 expression in tumoral cells and CD34 expression in peritumoral stroma, along with the absence of CEA androgen receptor and Periodic Acid-Schiff (PAS) expressions may support a diagnosis of DTE and vice versa. [2],[3],[4] So far, CK20 is the most reliable immunohistochemical marker in differentiating DTE from morphea-like BCC. [4] However, CK 20 expression in DTEs may be focal. [2],[3],[4]
Once the diagnosis is established, DTE may be clinically followed-up with an expectant policy. [1] Cryotherapy, dermabrasion or laser surgery may pose risks of recurrence and/or scar formation. Imiquimod has been used in two cases as an adjunctive therapeutic measure, but without apparent benefit. [5] In equivocal cases, the best treatment is complete surgical excision. [1] If there is a consideration of microcystic adnexal carcinoma or morphea-like BCC or if tissue preservation is crucial, Mohs micrographic surgery may be recommended. [1],[2]
| 1. |
Moynihan GD, Skrokov RA, Huh J, Pardes JB, Septon R. Desmoplastic trichoepithelioma. J Am Acad Dermatol 2011;64:438-9.
[Google Scholar]
|
| 2. |
Mamelak AJ, Goldberg LH, Katz TM, Graves JJ, Arnon O, Kimyai-Asadi A. Desmoplastic trichoepithelioma. J Am Acad Dermatol 2010;62:102-6.
[Google Scholar]
|
| 3. |
Jedrych J, Leffell D, McNiff JM. Desmoplastic trichoepithelioma with perineural involvement: A series of seven cases. J Cutan Pathol 2012;39:317-23.
[Google Scholar]
|
| 4. |
Costache M, Bresch M, Böer A. Desmoplastic trichoepithelioma versus morphoeic basal cell carcinoma: A critical reappraisal of histomorphological and immunohistochemical criteria for differentiation. Histopathology 2008;52:865-76.
[Google Scholar]
|
| 5. |
Seo SH, Kim GW, Sung HW. Imiquimod as an adjuvant treatment measure for desmoplastic trichoepithelioma. Ann Dermatol 2011;23:229-31.
[Google Scholar]
|
Fulltext Views
1,810
PDF downloads
1,892





![[Figure - 1]](#fig_ijdvl_2013_79_6_847_120754_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2013_79_6_847_120754_f2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2013_79_6_847_120754_f3.jpg){kind=link}