Translate this page into:
Palmar cutaneous metastasis from carcinoma cervix
2 Department of Obstetrics and Gynecology, JIPMER, Pondicherry - 605 006, India
3 Department of Pathology, JIPMER, Pondicherry - 605 006, India
4 Department of Radiotherapy, JIPMER, Pondicherry - 605 006, India
Correspondence Address:
Vikram Kate
Professor of Surgery, JIPMER, Pondicherry - 605 006
India
| How to cite this article: Elamurugan T P, Agrawal A, Dinesh R, Aravind R, Naskar D, Kate V, Reddy R, Elamurugan S, S, Basu D, P. Palmar cutaneous metastasis from carcinoma cervix. Indian J Dermatol Venereol Leprol 2011;77:252 |
Abstract
Carcinoma of the uterine cervix is the most common gynecological malignancy in developing countries. However, its cutaneous metastasis is a rare entity. The reported incidence of cutaneous metastasis ranges from 0.1 to 2%. Frequent sites of cutaneous metastasis in decreasing order are: abdominal wall, vulva and anterior chest wall. To the best of our knowledge, only three cases of cutaneous metastasis to the upper extremity have been reported in the world. We report a case of a 74-year-old postmenopausal lady diagnosed to have carcinoma cervix (stage IIIB) who presented with cutaneous metastasis to palm and thigh, 10 months after radical radiotherapy. At presentation, the primary disease had resolved completely. She had a small nodular growth in the left palm and left thigh. Fine needle aspirate cytology and core needle biopsy from both the nodular lesions were positive for squamous cell carcinoma.Introduction
Carcinoma of the uterine cervix is the most common gynecological malignancy in developing countries. It metastasizes mainly to lungs, bone and liver. [1] Cutaneous metastases from carcinoma cervix are extremely rare and are invariably a preterminal event. [2] The most common metastatic tumors to skin are from the breast, large intestine, lung and the ovary. [3] The reported incidence of cutaneous metastasis in carcinoma cervix is 0.1-2%, with abdominal wall, vulva, and anterior chest wall being the common sites. [4] To the best of our knowledge, only three cases of carcinoma cervix metastasizing to upper extremity have been reported all over the world and none have been reported in the palmar region. We report a case of carcinoma cervix metastasizing to palm and thigh.
Case Report
A 74-year-old postmenopausal lady had reported to Department of Obstetrics and Gynecology at our institute in June 2008, with complaints of bleeding per vagina for the preceding 6 months. She was diagnosed to have carcinoma of cervix, FIGO stage IIIB. Histologically, the patient had large cell non-keratinizing squamous cell carcinoma. The patient received external beam radiation to the whole pelvis, 50 Gy in 25 fractions by four-field box technique for 5 weeks followed by two intracavitary radiotherapy insertions of 6 Gy each at weekly intervals. At 8 months post RT, the patient had a complete response and was on regular follow-up since then.
A year after her index presentation, she presented to the Department of Surgery with complaints of a gradually increasing nodular growth in the left palm and left thigh, associated with pain, for 2 months. On examination of left palm, it showed a firm, 4 Χ 4 cm, tender, mobile and nodular subcutaneous lesion. Left thigh had a 3 Χ 3 cm, tender, firm, and mobile subcutaneous nodular lesion in the anterior aspect of lower third of thigh. Per speculum and per vaginal examination showed no evidence of loco-regional recurrence.
Fine needle aspirate cytology (FNAC) from both the nodular growths showed malignant squamous cells. Core needle biopsy from palmar lesion showed a cellular tumor with pleomorphic malignant squamous cells [Figure - 1]. Focally, keratin pearl formation was seen [Figure - 2]. A diagnosis of metastatic squamous cell carcinoma was made. The tumor cells were positive for pancytokeratin [[Figure - 2], inset]. Her complete hemogram, biochemistry profile, chest X-ray, ultrasound abdomen were normal. At 1 week follow-up, nodular lesion in the palm showed an ulcer with growth at the site of needle biopsy. At 1 month, the entire nodular lesion turned into an ulceroproliferative lesion of size 10 Χ 8 cm [Figure - 3] with areas of hemorrhage.
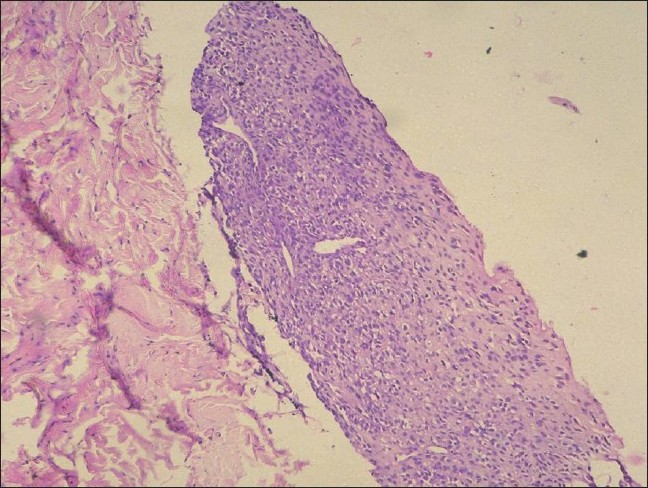 |
| Figure 1: Trucut biopsy of the swelling shows a cellular tumor with a fibroblastic stroma (H and E, �100) |
 |
| Figure 2: Higher magnification field showing malignant squamous cells with focal keratin pearl formation (arrow) (H and E, ×200). Inset shows that the tumor cells were pancytokeratin positive (IHC panCK, ×200) |
 |
| Figure 3: Ulceroproliferative lesion in the left palm |
Discussion
Distant metastasis from carcinoma cervix occurs commonly to lung, liver, and bone. [1] Cutaneous metastasis from carcinoma cervix is an unusual entity. Brady et al. in a series of 695 patients reported 0.1% incidence, while in another larger series of 1190 patients, 1.3% incidence of skin metastasis was reported. [4],[5] It is believed that the route of metastasis from cervix to the skin is lymphatic dissemination as tumor cells were found in the dilated lymphatics in skin lesions. [2],[4] The frequent sites of cutaneous metastasis in decreasing order are abdominal wall, vulva and anterior chest wall. [4] To the best of our knowledge, about 25 such cases have been reported in literature, [4],[6],[7],[8],[9] out of which only 3 cases had metastasis to the upper extremity. In our case, the metastatic lesion was in the palm which was a rare finding. The histological types that most commonly give rise to cutaneous metastasis are adenocarcinoma and undifferentiated carcinoma, whereas squamous cell carcinoma rarely does [4] as in this case. Cutaneous metastasis usually presents in three main forms - nodule, plaque and inflammatory telangiectasia. [4] In our case, the lesion was nodular at onset and progressed to an ulceroproliferative lesion which might have been due to the injury by needle biopsy. FNAC may be useful in diagnosing nodular lesion, but biopsy is required for plaque and telangiectatic lesions. [4] In our case, FNAC could give the diagnosis of metastatic carcinoma but needed confirmation with the help of needle biopsy.
We give the following explanation for stating this lesion as a metastatic one rather than a de novo lesion. First, occurrence of two primaries in a same patient is rare and hence the possibility of metastasis was considered. Second, the lesion was nodular and subcutaneous at onset, which became ulceroproliferative after the needle biopsy. Primary squamous cell carcinoma usually arises as a cutaneous ulcer or ulceroproliferative growth and not as a nodular subcutaneous swelling. Though the histology of the palmar lesion showed focal keratinization in contrast to the cervical histology which was non-keratinizing, this might have been due to sampling at the time of cervix biopsy.
The mean interval between the diagnosis of cervical cancer and the diagnosis of cutaneous metastasis is 16.9 months (0-69 months). [4],[10] In our case, the lesion appeared 10 months following RT. Cutaneous metastasis in carcinoma cervix is usually associated with preterminal advanced disease or recurrence at primary with multiple distant metastasis. [2] In the case reported here, the cutaneous metastasis appeared as the only isolated site of distant metastasis with no local recurrence. The main modality of treatment for patients with cutaneous metastasis from cervical carcinoma has been extirpation followed by radiotherapy. [4] Our patient was planned for below elbow amputation for palm lesion as a palliative measure and radiotherapy for thigh lesion, but the patient was lost to follow-up. Prognosis for such cases are poor as cutaneous metastasis is considered as a hallmark for preterminal disease, the mean survival being 3 months and survival for more than 1 year is seen in only 20% patients. [2],[4],[9]
| 1. |
Carlson V, Delclos L, Fletcher GH. Distant metastasis in squamous cell carcinoma of the uterine cervix. Radiology 1967;88:961-6.
[Google Scholar]
|
| 2. |
Malfetano JH. Skin metastasis from cervical cancer: A fatal event. Gynecol Oncol 1986;24:177-82.
[Google Scholar]
|
| 3. |
Krumerman MS, Garret R. Carcinoma metastatic to the skin. NY State J Med 1977;77:1900-3.
[Google Scholar]
|
| 4. |
Imachi M, Tsukamoto N, Kinoshita S, Nakano H. Skin metastasis from carcinoma of uterine cervix. Gynecol Oncol 1993;48:349-54.
[Google Scholar]
|
| 5. |
Brady LW, O'Neill EA, Farber SH. Unusual sites of metastasis. Semin Oncol 1977;4:59-64
[Google Scholar]
|
| 6. |
Behtash N, Ghaemmaghami F, Yarandi F, Ardalan FA, Khanafshar N. Cutaneous metastasis from carcinoma of the cervix at the drain site. Gynecol Oncol 2002;85:209-11.
[Google Scholar]
|
| 7. |
Copas PR, Spann CO, Thoms WW, Horowitz IR. Squamous cell carcinoma of the cervix metastatic to drain site. Gynecol Oncol 1995;56:102-4.
[Google Scholar]
|
| 8. |
Pertzborn S, Buekers TE, Sood AK. Hematogenous skin metastasis from cervical cancer at primary presentation. Gynecol Oncol 2000;76:416-7.
[Google Scholar]
|
| 9. |
Khurana R, Singh S. Isolated cutaneous metastasis to thigh from Cancer Cervix - 14 Years after curative radiotherapy. Internet J Gynecol Obstet 2009;11:1.
[Google Scholar]
|
| 10. |
Palaia I, Angioli R, Cutillo G, Manci N, Panici PB. Skin relapse from cervical cancer. Gynecol Oncol 2002;87:155-6.
[Google Scholar]
|
Fulltext Views
2,736
PDF downloads
2,466





![[Figure - 1]](#fig_ijdvl_2011_77_2_252_77486_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2011_77_2_252_77486_f2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2011_77_2_252_77486_f3.jpg){kind=link}