Translate this page into:
Partial dysautonomia: An interesting presentation
2 Department of Ophthalmology, University College of Medical Sciences, Guru Teg Bahadur Hospital, New Delhi, India
Correspondence Address:
Chander Grover
Department of Dermatology and STD, University College of Medical Sciences and GTB Hospital, New Delhi - 110 095
India
| How to cite this article: Kaul S, Grover C, Das GK. Partial dysautonomia: An interesting presentation. Indian J Dermatol Venereol Leprol 2017;83:596-598 |
Sir,
We report an interesting case with unilateral flushing and hyperhidrosis diagnosed to have an uncommon presentation of harlequin sign with Holmes–Adie syndrome.
A 45-year-old lady presented with a 15-year history of profuse sweating from the right half of her scalp, face, and neck with episodes of ipsilateral flushing associated with an uncomfortable sensation of warmth on the contralateral side. The intensity of sweating had progressed over the years to unbearable proportions. Simultaneously, she developed pain at the back of neck with restricted motion, along with episodic right-sided headache and difficulty in fixing gaze for prolonged periods. There was no history of trauma or any significant illness.
Examination at rest was unremarkable. However, post heat exposure or exertion, a distinct erythema and hyperhidrosis confined to right side of face, neck, and scalp with a sharp midline demarcation, was seen [Figure - 1]. Starch-iodine testing demonstrated anhidrosis on the left forehead [Figure - 2]. Ophthalmological examination revealed the presence of anisocoria [Figure - 3] with a right sided, irregularly dilated, tonic pupil (sluggish response to light or accommodation as compared to the normal left pupil). Upon instilling pilocarpine (0.1%) drops, the tonic pupil was seen to constrict much more than the normal left pupil. Neurological evaluation revealed bilateral hyporeflexic biceps and supinator tendon responses and absence of triceps, knee, and ankle deep tendon reflexes with a normal plantar response. Power for all major muscles groups was normal. Magnetic resonance imaging (MRI) of the cervical spine showed a diffuse disc bulge at C3/C4 level causing indentation of thecal sac and effacement of bilateral exiting nerve roots. Blood investigations including folate levels, rapid plasma reagin (RPR) test and autoimmune profile were normal.
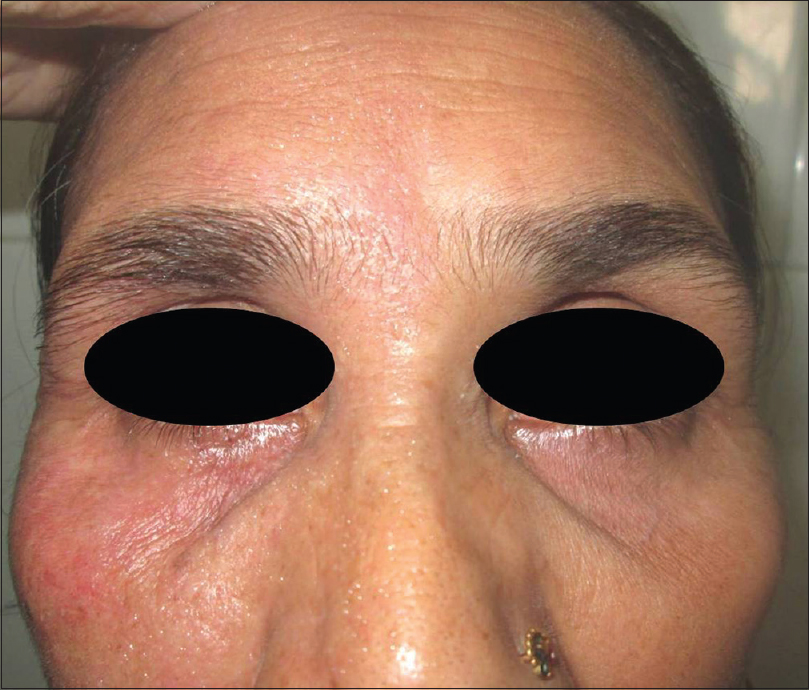 |
| Figure 1: Right sided flushing and hyperhidrosis as noticed on the face |
 |
| Figure 2: Starch iodine test demonstrating anhidrosis on the left half of forehead |
 |
| Figure 3: Right sided pupil showing irregular outline. It is also larger (tonically dilated) as compared to left pupil |
Considering her presentation, she was diagnosed as partial dysautonomia in the form of harlequin sign with Holmes-Adie syndrome. She was explained the benign nature of her condition, advised to avoid extreme temperature and prescribed topical aluminium chlorohydrate 20% lotion at night during summer. The patient has remained comfortable for the past year.
Partial dysautonomia is characterized by abnormal regulation of the autonomic nervous system, resulting in symptoms like focal or generalized decrease in sweating, flushing, orthostatic hypotension, aberrant ocular responses and altered cardiovascular reflexes occurring either as isolated primary or secondary phenomenon, or as a combination.[1] It is an uncommon condition, which although essentially benign, can be extremely debilitating.
Among the major partial dysautonomic syndromes are the harlequin syndrome, described by Lance et al. in 1988. It is a rare disorder of sympathetic dysfunction characterized by unilateral hypohidrosis with contralateral flushing of face in response to physical exertion or heat.[2] It can occur as an isolated anomaly, or in association with other dysautonomic syndromes. A recent review of 108 cases found that 44.4% cases had harlequin syndrome alone; while 35.1% cases presented with Horner's syndrome. The association with Holmes-Adie syndrome, as seen in our case, is distinctly uncommon (5.5% cases).[3] Known causes of acquired disease include space occupying lesions like mediastinal neurinoma, thoracic neurofibroma, cervical syrinx, intramedullary astrocytoma, along with iatrogenic causes viz. jugular vein catheterization, paravertebral thoracic blocks, thoracic sympathectomy, etc.[4]
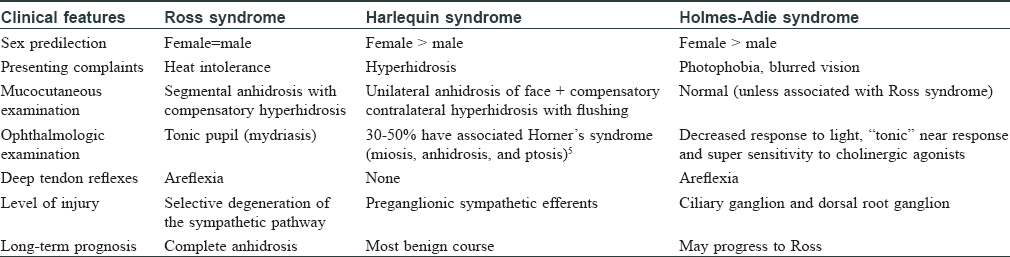
Ross syndrome and Holmes–Adie syndrome are rarer syndromes whose salient features are presented in [Table - 1].
In these cases, the pathology lies on the anhidrotic side and is due to a disruption of the sympathetic nervous system. The result is compensatory flushing and hyperhidrosis contralaterally.[5] The constellation of signs and symptoms offer a clue to the level of sympathetic damage. A combination of harlequin sign with Horner's syndrome points towards a lesion of the superior cervical ganglion, whereas harlequin sign with Ross or Holmes-Adie syndrome implicates an anomalous postganglionic cholinergic parasympathetic and sympathetic system response (supplying the iris smooth muscles and the eccrine glands).[5] This also leads to decreased ipsilateral cutaneous blood flow. Any vasodilatory signal thus result in ipsilateral pallor due to the vasoconstriction, giving a flushed appearance on the contralateral side with a definite midline demarcation.
Hyperhidrosis can be a very distressing complaint, as in our patient. Various management options have been described for this. If general measures of avoiding warm ambient temperatures and excessive exertion are deemed insufficient or not practical by the patient, they could be prescribed topical antiperspirant preparations. In severe cases, botulinum toxin may also be advised. Surgical sympathectomy is reserved for severe cases, unresponsive to above measures. Our patient found the use of topical antiperspirant lotion acceptable and relieving.
This case serves to sensitize dermatologists to this uncommon association. A comprehensive neurological and ophthalmological investigation is warranted along with a need to rule out malignancies in late onset cases. For idiopathic disease, counseling may prove sufficient but treatment modalities should be discussed and offered, if the need arises.
Declaration of patient consent
The patient has given her Verbal consent for her images and other clinical information to be reported in the journal. The patient understand that her name and initial will not be published and due efforts will be made to conceal her identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
| 1. |
Bacon PJ, Smith SE. Cardiovascular and sweating dysfunction in patients with Holmes-Adie syndrome. J NeurolNeurosurg Psychiatry 1993;56:1096-102.
[Google Scholar]
|
| 2. |
Lance JW, Drummond PD, Gandevia SC, Morris JG. Harlequin syndrome: The sudden onset of unilateral flushing and sweating. J NeurolNeurosurg Psychiatry 1988;51:635-42.
[Google Scholar]
|
| 3. |
Guilloton L, Demarquay G, Quesnel L, De Charry F, Drouet A, Zagnoli F. Dysautonomic syndrome of the face with harlequin sign and syndrome: Three new cases and a review of the literature. Rev Neurol (Paris) 2013;169:884-91.
[Google Scholar]
|
| 4. |
Willaert WI, Scheltinga MR, Steenhuisen SF, Hiel JA. Harlequin syndrome: Two new cases and a management proposal. ActaNeurolBelg 2009;109:214-20.
[Google Scholar]
|
| 5. |
Kaur S, Aggarwal P, Jindal N, Dayal S, Jairath V, Jain VK, et al. Harlequin syndrome: A mask of rare dysautonomic syndromes. Dermatol Online J 2015;21. pii: 13030/qt3q39d7mz.
[Google Scholar]
|
Fulltext Views
3,423
PDF downloads
868





![[Figure - 1]](#fig_ijdvl_2017_83_5_596_211618_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2017_83_5_596_211618_f2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2017_83_5_596_211618_f3.jpg){kind=link}
![[Table - 1]](#tbl_ijdvl_2017_83_5_596_211618_t4.jpg){kind=link}