Translate this page into:
Patch test results from a contact dermatitis clinic in North India
Correspondence Address:
Sanjeev Handa
Department of Dermatology, Venereology and Leprology, Postgraduate Institute of Medical Education and Research, Chandigarh, Punjab
India
| How to cite this article: Handa S, Jindal R. Patch test results from a contact dermatitis clinic in North India. Indian J Dermatol Venereol Leprol 2011;77:194-196 |
Sir,
Contact dermatitis is an increasing problem all over the world and accounts for 4-7% of all dermatological consultations. [1] The allergens which are included in standard series vary from country to country based on the local experience. Here we present the prevalence and pattern of contact allergy in patients attending our contact dermatitis clinic. Clinic records of 560 patients of suspected allergic contact dermatitis attending the contact dermatitis clinic at PGIMER Chandigarh, a tertiary care centre in North India, were analyzed. Details regarding age, sex, duration of illness, occupation, clinical diagnosis, sites affected, and history of atopy were recorded using the predesigned proforma. Initial 247 patients were tested with European Standard Series (ESS) and rest with Indian Standard Series (ISS). Plant antigens (parthenium, xanthium, sunflower, chrysanthemum, and marigold) and vegetables (garlic, onion and tomato) were also routinely tested along with patients own antigens like hair dye and cosmetics as indicated by the history.
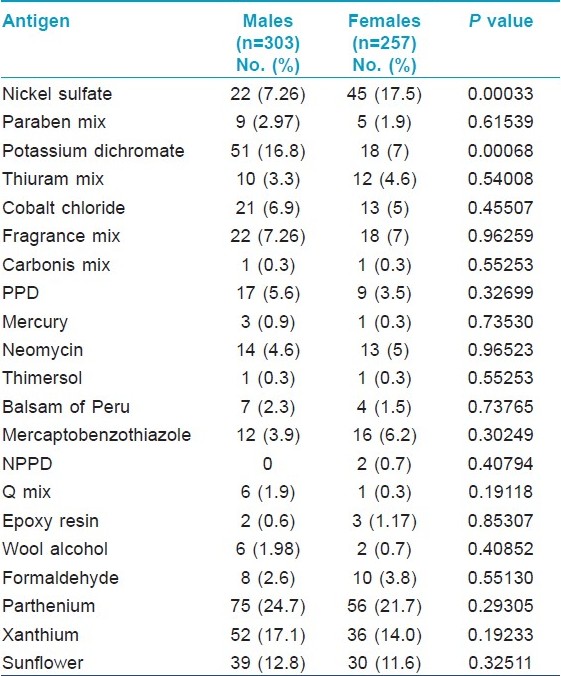
Out of a total of 560 patients patch tested over a 6 year period, 303 (54.1%) were males and 257 (45.9%) were females with age ranging from 9 to 85 years (mean 40±0.6 years). The duration of disease ranged from 1 to 420 months with a mean of 41±2.2 months. Air-borne contact dermatitis (ABCD) affecting face, neck, flexures of arms, and legs was the most common pattern seen in 165 patients. Out of these 20 (12%) patients had photo-aggravation. Localized allergic contact dermatitis was the next common diagnosis (133 patients) followed by hand dermatitis (90 patients) and footwear dermatitis (51 patients). Hand and foot dermatitis together was seen in 22 patients. A picture resembling chronic actinic dermatitis (CAD) was seen in 15 patients. Three hundred fifty-three (63%) patients showed positivity to one or more allergens. Nickel sulfate (17.5%) was the most common sensitizing agent in females followed by potassium dichromate (7%), fragrance mix (7%) and mercaptobenzothiazole (6.2%). In males, potassium dichromate (16.8%) was the most common allergen and next in frequency were nickel sulfate (7.26%), fragrance mix (7.26%), and cobalt chloride (6.9%) [Table - 1]. The difference in sensitivity to nickel between males and females was found to be statistically significant (P= 0.00033) as was that to potassium dichromate (P=0.00068). Among the plant allergens tested, maximum positive reactions were due to parthenium (23.5%) and xanthium (15.8%). Personal or family history of atopy was found in 186 (30%) patients. However, there was no statistically significant difference in contact sensitization between atopics and non-atopics.
This study was designed to evaluate the rates of sensitivity of Indian patients to various allergens presenting to the contact dermatitis clinic of a tertiary care centre. In this study, 63% patients showed sensitivity to one or more allergens. This figure is comparable to that reported by Davoudi et al, Bajaj et al, and also our previous report but much higher than that reported by a recent study from Turkey (32.3%). [2],[3],[4],[5] This difference could be explained by the fact that our data is of a contact dermatitis clinic at a referral center where patients suspected of having allergic contact dermatitis were subjected to patch testing increasing the probability of a positive result. A comparison of positivity rates to different allergens as reported by recent Indian studies has been shown in [Table - 2].
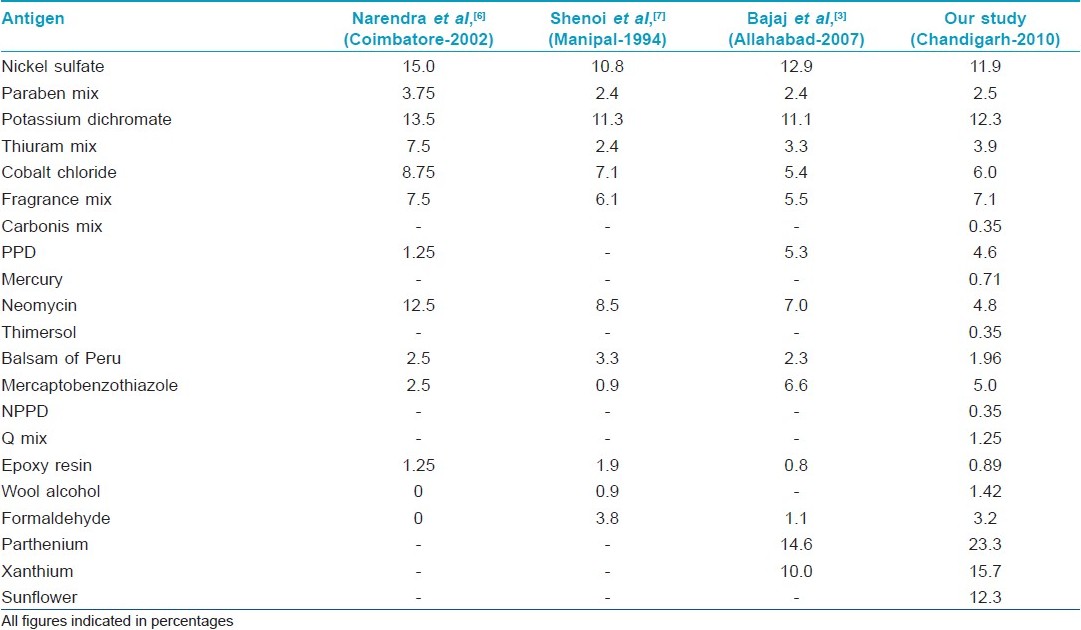
The overall sensitization rates of males and females did not differ significantly but the differences were significant for nickel and potassium dichromate individually. Females were more sensitive to nickel and males to potassium dichromate. Five most common allergens in our study were: potassium dichromate (12.3%), nickel (11.9%), fragrance mix (7.14%), cobalt chloride (6.07%), and mercaptobenzothiazole (5%). Most common sensitizer in plant series was parthenium hysterophorus (23.5%), followed by xanthium (15.8%) and sunflower (12.3%). Similar high rates of parthenium (14.6%) and xanthium (10%) sensitivity were also reported by Bajaj et al. [3] Traditionally parthenium dermatitis is reported to have male predominance especially in farming countries. However in our study both males and females were equally affected. Rampant overgrowth of this plant in the cities and suburbs could possibly explain the increased contact sensitivity in housewives and people of profession other than agriculture.
In conclusion, in our region rates of sensitivities to specific allergens have not changed much as is evident by comparison with the previous study from our centre. [4] Parthenium remains the most common cause of ABCD with both males and females presenting with equal frequency. Apart from plant antigens potassium dichromate and nickel are very common sensitizers. Testing with standard series is very essential to identify the cause of contact dermatitis but these must be reviewed frequently so that the infrequent allergens can be discarded and other relevant ones can be added.[7]
| 1. |
Mendenhall RG, Ramsay DL, Girard RA. A study of the practice of dermatology in the United States. Arch Dermatol 1978;114:1456-62.
[Google Scholar]
|
| 2. |
Davoudi M, Firoozabadi MR, Gorouhi F, Zarchi AK, Kashani MN, Dowlati Y, et al. Patch testing in Iranian patients: A ten-year experience. Indian J Dermatol 2006;51:250-4.
[Google Scholar]
|
| 3. |
Bajaj AK, Saraswat A, Mukhija G, Rastogi S, Yadav S. Patch testing experience with 1000 patients. Indian J Dermatol Venereol Leprol 2007;73:313-8.
[Google Scholar]
|
| 4. |
Sharma VK, Chakrabarti A. Common contact sensitizers in Chandigarh, India. A study of 200 patients with the European standard series. Contact Dermatitis 1998;38:127-31.
[Google Scholar]
|
| 5. |
Akasya-Hillenbrand E, Ozkaya-Bayazit E. Patch test results in 542 patients with suspected contact dermatitis in Turkey. Contact Dermatitis 2002;46:17-23.
[Google Scholar]
|
| 6. |
Narendra G, Srinivas CR. Patch testing with Indian standard series. Indian J Dermatol Venereol Leprol 2002;68:281-2.
[Google Scholar]
|
| 7. |
Shenoi DS, Srinivas CR, Balachandran C. Results of patch testing with a standard series of allergens at Manipal. Indian J Dermatol Venereol Leprol 1994;60:133-5.
[Google Scholar]
|
Fulltext Views
3,105
PDF downloads
1,800





![[Table - 1]](#tbl_ijdvl_2011_77_2_194_77465_b1.jpg){kind=link}
![[Table - 2]](#tbl_ijdvl_2011_77_2_194_77465_b2.jpg){kind=link}