Translate this page into:
Pattern of skin diseases in Kumaun region of Uttarakhand
Correspondence Address:
Saurabh Agarwal
Department of Skin and VD, Government Medical College, Haldwani (Nainital), Uttarakhand-263 139
India
| How to cite this article: Agarwal S, Sharma P, Gupta S, Ojha A. Pattern of skin diseases in Kumaun region of Uttarakhand. Indian J Dermatol Venereol Leprol 2011;77:603-604 |
Sir,
India is a large country with diversity in social, economic, racial, geographic, and environmental factors; therefore we have different patterns of skin diseases in various regions of the country. A number of workers have reported pattern of skin diseases in different areas from India, but there is no such report from Uttarakhand so far. Uttarakhand state, which is situated in northwest region of India, is divided in two regions, namely, Kumaun and Garhwal. Kumaun division is comprised of six districts, namely, Nainital, Almorah, Bageshwar, Champawat, Udham Singh Nagar, and Pithoragarh. Government Medical College, Haldwani (Nainital) is one of the referral centers for Kumaun division. The average rainfall in Uttarahkand is 1397.0 mms and temperature varies from -2.7 °C to 41.5°C. There is forest area of 34651 sq. km out of 53483 sq. km geographical area. It is a hilly state with many districts situated at an altitude of 2000 m or above. Humidity is low. About 75% population is involved in agricultural or forestry work. To know the pattern of skin diseases in this region, the data of all the new skin patients attending the skin OPD during the period of 5 years starting from 1 st January 2006 to 31 st December 2010 was analyzed retrospectively from outpatient registers. The demographic profile of these patients including age and sex distribution was noted. Diagnosis of various skin diseases was made on clinical grounds and relevant investigations were done whenever required.
Skin patients comprised of 6.16% of all the cases who attended the hospital in this period. A total of 28,842 new skin patients with different dermatological diseases were seen during study period. 15,589 (54.05%) of the patients were male and 13,253 (45.96%) were female with a male/female ratio of 1.18:1. Age distribution shows that majority of the patients were in age group 21-30 year with 7735 (26.82%) cases followed by 11-20 year age group with 6299 (21.84%) cases. 16847 (58.7%) patients were having non-infective skin diseases while only 7813 (27.1%) patients were suffering from infective skin diseases [Table - 1]. Fifteen percent patients were categorized under miscellaneous group. Eczemas (19.9%) emerged as largest group of skin diseases in noninfective skin diseases group. Hand eczema (23.4%) was most common in eczemas. Acne comprised of 10% cases while other noninfective skin diseases were melasma (4.75%), psoriasis (3.95%), polymorphous light eruption (PMLE) (3.81%), urticaria (3.59%), vitiligo (2.62%), diffuse hair loss (1.79%), lichen planus (1.77%), alopecia areata (1%). Fungal infections (10.7%) were most common in infective skin diseases group. In superficial fungal infections, dermatophytosis (71.5%) was most common followed by P. versicolor (18.6%) and candidiasis (6.7%). In deep mycoses, 25 cases of sporotrichoses, 6 cases of chromoblastomycoses and 4 cases of mycetoma were seen. In viral infections, verruca vulgaris (40%) was most common followed by herpes zoster (22.9%), varicella (15.4%), molluscum contagiosum (14.3%), and herpes simplex infection (7.4%). Surprisingly cases of pyodermas were only 1.84%. Sexually transmitted diseases (STD′s) and leprosy comprised of 1.34% and 1.28% cases, respectively.
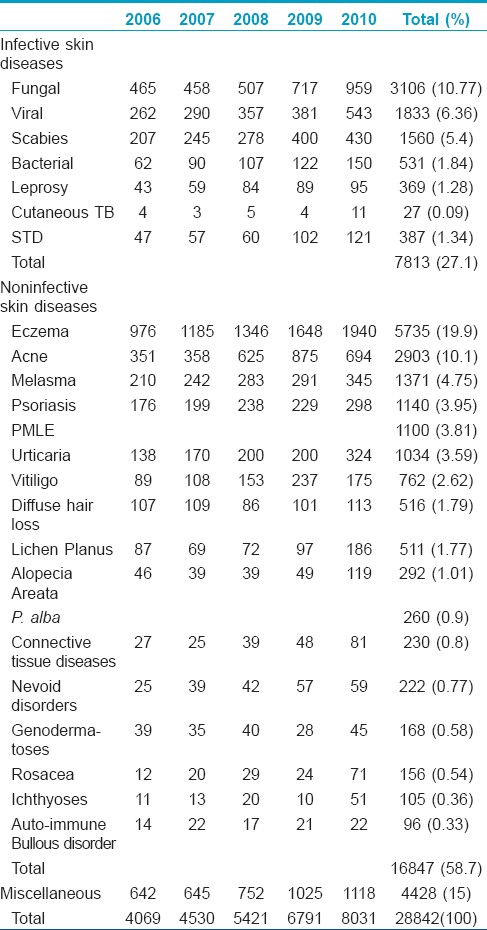
The prevalence of noninfective skin diseases has outstripped that of infective skin diseases in some studies varying from 40.9% to 55.3%. [1],[2],[3] Further, this trend was noticed in our present study with non-infective skin diseases accounting for 58.7% cases. However, some other studies have reported higher prevalence of infective skin diseases varying from 35.2% to 59.1%. [4] In contrast infective skin diseases accounted for only 27.1% cases in our present study. This variance could possibly be due to differing susceptibilities in different population groups in diverse geographical regions. Low population density (189 per sq. km) and high literacy rate (79.6%) in Uttarakhand could have affected also. Comparatively lower prevalence of fungal infection in present study can be attributed low humidity in this region. Contrary to this, 25 cases of sporotrichosis were seen in the study period of 5 years from this region. In India, the Himalayan foothill regions, where there is heavy rainfall and moderate temperatures, seem to form a belt from where reports of sporotrichosis are frequent. Pyodermas comprised of only 1.84% cases in this study in contrast to many others who have reported higher prevalence. [1] It could be explained due to easy diagnosis and therefore treatment given by general practitioners and also frequent self use of antibiotics by the patients. Viral infections accounted for 6.4% cases and formed second largest group in infective skin diseases, though other studies have reported lower prevalence of viral infections varying from 1.15% to 4.69%. [1],[2],[4],[5] High prevalence of melasma (4.75%) and PMLE (3.91%) could be due to high altitude and more outdoor activities.
Acknowledgment
We are thankful to medical record section, Government Medical College, Haldwani (Nainital) for providing yearwise total number of patients who attended the hospital OPD.
| 1. |
Das KK. Pattern of dermatological diseases in Guwahati medical college and hospital Guwahati. Indian J Dermatol, Venereol Leprol 2003;69:16-8.
[Google Scholar]
|
| 2. |
Devi T, Zamzachin G. Pattern of skin diseases in Imphal. Indian J Dermatol 2006;51:149-50.
[Google Scholar]
|
| 3. |
Asokan N, Prathap P, Ajithkumar K, Ambooken B, Binesh BG, George S. Pattern of skin diseases among patients attending a tertiary care teaching hospital in Kerala. Indian J Dermatol 2009;75:517-8.
[Google Scholar]
|
| 4. |
Grover S, Ranyal RK, Bedi MK. A cross section of skin diseases in rural Allahabad. Indian J Dermatol 2008;53:179-81.
[Google Scholar]
|
| 5. |
S, Nair TV Gopalakrishnan. Pattern of dermatological diseases in Trivandrum. Indian J Dermotol Venereol Leprol 1999;65:261-3.
[Google Scholar]
|
Fulltext Views
3,482
PDF downloads
2,193





![[Table - 1]](#tbl_ijdvl_2011_77_5_603_84073_b1.jpg){kind=link}