Translate this page into:
Pentazocine induced ulceration of the buttocks
Correspondence Address:
Sushruta Kathuria
Department of Dermatology and Venereology, AIIMS, New Delhi - 110 029
India
| How to cite this article: Kathuria S, Ramesh V, Singh A. Pentazocine induced ulceration of the buttocks. Indian J Dermatol Venereol Leprol 2012;78:521 |
An 18-year-old-girl presented with indurated erythematous plaques, nodules, discharging sinuses and ulcers localized to the buttocks for 2 years. On examination, discharge from the sinuses was minimal, and the nodules were better felt than seen, firm to hard on palpation and slightly tender [Figure - 1]. She also complained of recurrent abdominal pain for 3 years, refractory to oral analgesics and improved significantly only by injectable analgesics. The intramuscular injections were given on buttocks by the local practitioner once or twice daily and were continued even after occurrence of discharging sinuses. Investigations were carried out for abdominal pain such as routine blood chemistries, hemogram, ultrasound of abdomen and pelvis, and no cause could be detected for the abdominal pain. Wedge biopsy from edge of ulcer showed irregular acanthosis, mild perivascular infiltrate of lymphocytes, histiocytes with some siderophages and focal dermal fibrosis [Figure - 2]. Subcutaneous fat showed lobular panniculitis, focal macro- and microcysts, lipophages and thickened septae with fibrosis [Figure - 3]. Special stains for acid fast bacilli, fungal hyphae and spores were negative. Multiple biopsies did not show growth of any organism. A morning urine sample was tested for pentazocine by thin layer chromatography (TLC) and was found positive. Patient was diagnosed as a case of pentazocine-induced ulceration and panniculitis. The patient was admitted and counseled regarding stopping pentazocine. During 2 weeks of hospital stay, abdominal pain had paradoxically improved by 90% with paracetamol 500 mg once daily. However, no change was seen in the pentazocine ulcers.
 |
| Figure 1: Multiple nodules and discharging sinuses on buttocks |
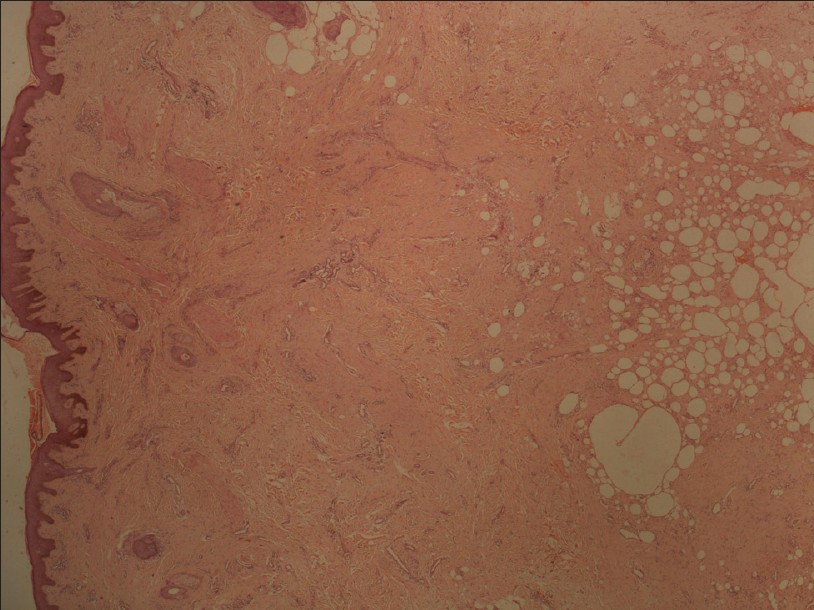 |
| Figure 2: Fibrosis in mid and lower dermis with panniculitis. (H and E, ×10) |
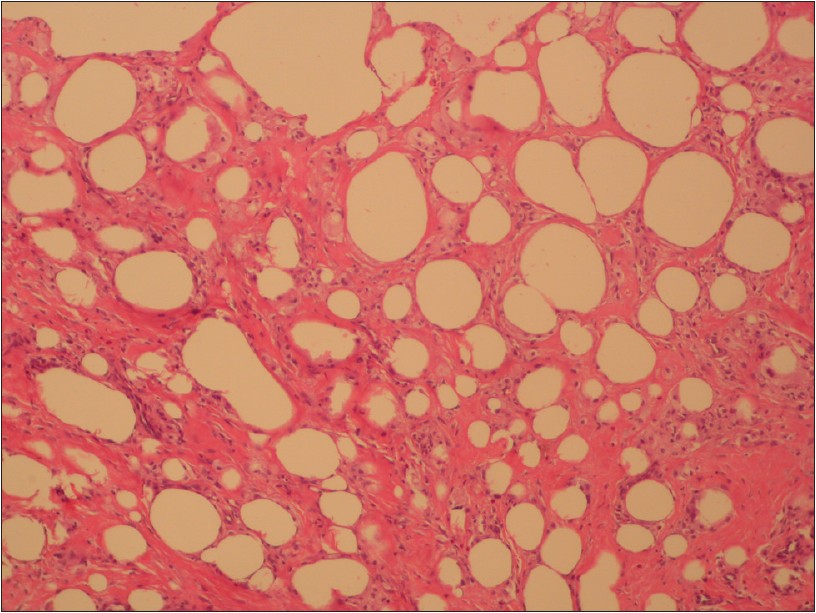 |
| Figure 3: Lobular panniculitis with fatty micro- and macrocysts and septal fibrosis. (H and E, ×40) |
Pentazocine is a non-narcotic, non-addicting analgesic, introduced in 1967. However, its addicting and dependence properties are known, [1] and complications due to its abuse have been reported. [2] The diagnosis of pentazocine dermopathy should be suspected in patients presenting with woody hard nodules or plaques and ulcerations with a history of chronic pain. Most patients either have direct access to pentazocine or procure from relatives, or are advised by medical practitioners. Clinical presentation can vary from irregular ulcers with surrounding induration or hyperpigmentation [2] to thrombophlebitis, [3] puffy hand syndrome, ulcers, nodules or scars along veins, [4] and fibrous papules arranged linearly. [5] Such patients unusually show less discomfort than expected even when the lesions are extensive. The ulcers often occur over sites easy for the patient to inject like thighs, arms, forearms, abdomen and most of the peripheral veins have become thrombosed due to repeated intravenous pentazocine injections. [4] When interrogated, they adamantly refuse knowledge and use of such injections. Sometimes, repeated questioning about severity of pain, treatment, occupation of the patient and family members may help in diagnosis. Admitting the patient, closely observing how the patient copes with pain and evolution of the ulcers, is often helpful as there will be no access to pentazocine.
In our case, patient repeatedly took analgesics for chronic epigastric pain of unknown cause, which gave us a clue to the diagnosis. Diagnosis was confirmed by exclusion of other diseases, demonstration of characteristic histopathology on skin biopsy and positive urine test for pentazocine. TLC on urine sample can detect pentazocine if consumed within last 72 hours, and in this patient, patient admitted to taking pentazocine a day before. Other causes of discharging sinuses with an induration include scrofuloderma, atypical mycobacterial infections, mycetoma, hidradenitis suppurativa and malakoplakia. Scrofuloderma, atypical mycobacterial infections and mycetoma were ruled out by absence of granulomas and mixed inflammatory infiltrate on biopsy. Further, no organism could be detected by special stains or culture. The characteristic sites like axillae and groin were spared, and histopathology did not show neutrophils, which ruled out hidradenitis suppurativa.
Pentazocine-induced ulcers are underrecognized cause of chronic non-healing ulcers, not only among dermatologists but also among clinicians of other specialities. The lesions increased as pentazocine was continued on an advice of local practitioner. Pentazocine is a commonly used drug for chronic pain, and this case highlights the importance of being aware of its pentazocine ulcers as the vital component of management is withdrawal of the abused drug, psychiatric counseling and alternative treatment for chronic pain.
| 1. |
Sandoval RG, Wang RIH. Tolerance and dependence on pentazocine. N Engl J Med 1969;280:1391-2.
[Google Scholar]
|
| 2. |
Parks DL, Perry HO, Muller SA. Cutaneous complications of pentazocine injections. Arch Dermatol 1971;104:231-5.
[Google Scholar]
|
| 3. |
Girolami A, Cella G. Acute superficial phlebitis in a patient with hemophilia A: Probably an iatrogenic effect. Acta Haematol 1972;48:307-11.
[Google Scholar]
|
| 4. |
Prasad HR, Khaitan BK, Ramam M, Sharma VK, Pandhi RK, Agarwal S, et al. Diagnostic clinical features of pentazocine-induced ulcers. Int J Dermatol 2005;44:910-5.
[Google Scholar]
|
| 5. |
De D, Dogra S, Kanwar AJ. Pentazocine induced leg ulcers and fibrous papules. Indian J Dermatol Venereol Leprol 2007;73:112-3.
[Google Scholar]
|
Fulltext Views
2,478
PDF downloads
2,594





![[Figure - 1]](#fig_ijdvl_2012_78_4_521_98104_u1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2012_78_4_521_98104_u2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2012_78_4_521_98104_u3.jpg){kind=link}