Translate this page into:
Porokeratotic eccrine ostial and dermal duct nevus
Correspondence Address:
Deeptara Pathak
C/O Dr. Raj Kubba, 10, Aradhana enclave, R.K. Puram, Sector-13, New Delhi 110066
India
| How to cite this article: Pathak D, Kubba R, Kubba A. Porokeratotic eccrine ostial and dermal duct nevus. Indian J Dermatol Venereol Leprol 2011;77:174-176 |
Abstract
Porokeratotic eccrine ostial and dermal duct nevus (PEODDN) is a rare variant of porokeratosis with characteristic histological feature of cornoid lamella involving the acrosyringium. We report a classic case of a 20-year-old male, who clinically presented to us with keratotic papules and plaque with pits, few having comedo like plugs, on right palm and sole since 1 year of age. A punch biopsy from palm was diagnostic as well as confirmatory showing cornoid lamella involving an eccrine duct which is the characteristic histopathological feature of PEODDN.Introduction
Porokeratotic eccrine ostial and dermal duct nevus (PEODDN) is a rare variant of porokeratosis which is a disorder of keratinization and clinically presents as asymptomatic localized area of plugged pits in a linear distribution on palm and soles or a generalized form having characteristic histological feature of cornoid lamella, which is a thin column of parakeratotic cells with an absent or decreased underlying granular layer and dyskeratotic cells that involve the acrosyringia. [1]
Case Report
A 20-year-old male presented with asymptomatic keratotic papules and plaques on right palm and right sole since 1 year of age. There was no family history of a similar condition.
Clinical examination showed gross morphologic features of keratotic papules (some discrete whilst others coalescing to form plaques in a linear configuration), distributed over right palm, extending from wrist area to thenar eminence and the palmar aspect of thumb and index finger. Few pits which had keratinous, comedo like plugs were seen in between the papules. Similar lesions were found on the right sole, extending from heel to medial aspect of foot as shown in [Figure - 1] and [Figure - 2]. Our clinical differential diagnosis was blaschkoid porokeratotic and linear verrucous epidermal nevus (VEN). General physical examination showed no abnormality. Patient was advised punch biopsy. The histopathological features were characteristic of PEODDN [Figure - 3], showing orthokeratosis, and parakeratotic column filling a deep cup shaped invagination in the epidermis. Epidermis at the base of column showed loss of granular cells replaced by cluster of dyskeratotic cells. An eccrine duct was seen at the base of invagination consistent with acrosyringeal origin. Patient was referred for ablative laser surgery.
 |
| Figure 1: Keratotic papules and plaque on right palm wrist area, thenar eminence, palmar aspect of thumb and index finger in a linear pattern. Few pits are seen in between the papules |
 |
| Figure 2: Keratotic papules and plaque with few pits having comedo like plugs on right sole extending from heel to medial aspect of foot |
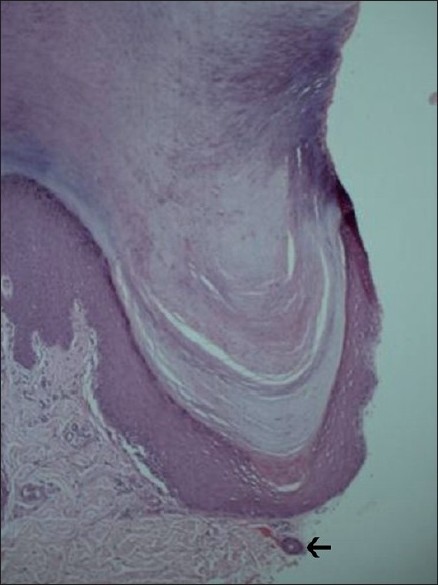 |
| Figure 3: Punch biopsy from palm shows cornoid lamella with underlying eccrine duct (arrow) (H and E, ×100) |
Discussion
PEODDN was initially coined by Marsden et al, as comedo nevus of palm and showed keratotic plugs occluding the eccrine ostia by scanning electron microscopy. It was later redefined by Abell and Reed in 1980. [1] There are also other synonyms used to describe PEODDN, such as linear eccrine nevus with comedons, palmar and plantar pseudocomedo porokeratotic sweat nevus, and porokeratotic eecrine ostial and hair follicle nevus. [2] The cause is still unknown. Earlier, it was hypothetized that it was an epidermal invagination which was widely dilated, keratin plugged acrosyringial duct with dermal duct continuing from the base. [2],[3],[4] Stoof et al, [3] proposed that the lack of carcinoembryonic antigen (CEA) expression by acrosyringial cells was due to abnormal development of the structure. [2] In recent years, immunohistochemistry with CEA staining the cuticle of the acrosyringium and dermal duct traversing the parakeratotic column but not the inner borders of the epidermal invagination, supports the theory that it represents an abnormally keratinizing epidermal invagination through which an acrosyryngium traverses. [1],[5],[6] Wang et al, [1] have demonstrated that abnormal keratinizing epidermal invagination may be due to increased proliferation as shown by keratin (Ki-67) staining at the basal layer underneath the cornoid lamella.
PEODDN clinically presents as either multiple linear punctuate pits with comedo like plugs on palms and soles or keratotic plaques and papules that resemble linear VEN on other areas. [1],[7] There are approximately 45 reported cases in literature till now. Majority of the cases are localized to palm and soles except few which have involvement of other areas like trunk, buttock and rare widespread involvement along Blaschko′s lines. Presentation of PEODDN distributed along Blaschko′s lines may be due to genetic mosaicism as postulated by Cambiaghi et al. [8] PEODDN can present at the time of birth or early childhood or can have a late onset. It is mostly asymptomatic but can be associated with pruritus, hyperhidrosis or anhidrosis. [1] There are rare case reports of PEODDN associated with conditions like hyperthyroidism and sensory polyneuropathy, breast hypoplasia, Bowen disease, deafness and development delay, seizure disorder, hemiparesis, scoliosis, alopecia, onychodysplasia and squamous cell carcinoma. [2],[4],[8],[9] It is unclear whether these associations are coincidental findings or have causal relationship. Coexistence of linear psoriasis has been reported and was hypothesized that it was due to somatic mutation in a rare gene which is in the spectrum of polygenic predisposition for psoriasis. [9]
Our case presented classically with asymptomatic localized involvement of right palm and sole with keratotic papules and plaques with few pits having in between comedo like plugs in a linear fashion without any association. Histopathology is diagnostic of PEODDN which shows epidermal invaginations containing cornoid lamella that involves the eccrine ducts. Our case also showed characteristic histopathological features of PEODDN. There are reports in literature where the cornoid lamella involves eccrine ducts and hair follicles. [1],[4],[10] Differential diagnosis includes linear VEN, inflammatory linear VEN, linear porokeratosis, linear psoriasis, punctuate keratoderma and nevus comedonicus. All the above diseases lack the characteristic histological feature of cornoid lamella involving eccrine duct. The lesions may persist or may become more hyperkeratosis or may involute with time.
There are very few options available regarding treatment, mentioned in the literature. Surgical excision is an option for small and localized lesions in appropriate anatomical location. CO 2 laser was found to be effective in a few cases. Ultrapulse CO 2 laser has a much better cosmetic outcome in comparison to surgical excision and conventional CO 2 laser, with minimal hypopigmentation and scaring. Topicals like keratolytics, retinoids, steroids, calcipotrial, and anthralin were found to be ineffective. Other modalities like phototherapy, cryotherapy, and electrocautery were found to have poor outcome. [3],[6],[7],[9],[10]
It is a rare disease in India and only one case report has been reported till date. [11] Biopsy is essential to make diagnosis and there is a need to identify new treatment options and to improve the existing options to do justice to this cosmetically disfiguring condition with psychological impact.
| 1. |
Wang NS, Meola T, Orlow SJ. Porokeratotic Eccrine ostial and Dermal Duct Nevus: A report of 2 cases and review of literature. Am J Dermatopathol 2009;31:582-6.
[Google Scholar]
|
| 2. |
Sassmannshausen J, Bogomilsky J, Chaffins M. Porokeratotic eccrine ostial and dermal duct nevus: A case report and review of literature. J Am Acad Dermatol 2000;43:364-7.
[Google Scholar]
|
| 3. |
Stoof T, Starink T, Nieboer C. Porokeratotic eccrine ostial and dermal duct nevus: Report of a case of adult onset. J Am Acad Dermatol 1989;20:924-7.
[Google Scholar]
|
| 4. |
Goddard DS, Rogers M, Frieden IJ, Krol AL, White CR Jr, Jayaraman AG, et al. Widespread porokeratotic adnexal ostial nevus: Clinical features and proposal of a new name unifying porokeratotic eccrine ostial and dermal duct nevus and porokeratotic eccrine and hair follicle nevus. J Am Acad Dermatol 2009;61:1060.e1-14.
[Google Scholar]
|
| 5. |
Soloeta R, Yanguas I, Lozano M, González-Güemes M, Goday JJ. Immunohistochemical study of porokeratotic eccrine nevus. Int J Dermatol 1996;35:881-3.
[Google Scholar]
|
| 6. |
Bergman R, Lichtig C, Cohen A, Friedman-Birnbaum R. Porokeratotic eccrine ostial and dermal duct nevus: An abnormally keratinizing epidermal invagination or a dilated, porokeratotically plugged acrosyringium and dermal duct. Am J Dermatopathol 1992;14:319-2.
[Google Scholar]
|
| 7. |
Leung CS, Tang WY, Lam WY, Lo KK. Porokeratotic eccrine ostial and dermal duct naevus with dermatomal trunk involvement: Literature review and report on the efficacy of laser treatment. Br J Dermatol 1998;138:684-8.
[Google Scholar]
|
| 8. |
Cambiaghi S, Gianotti R, Caputo R. Widespread porokeratotic eccrine ostial and dermal duct nevus along Blaschko lines. Pediatr Dermatol 2007;24:162-7.
[Google Scholar]
|
| 9. |
Yu HJ, Ko JY, Kwon HM, Kim JS. Linear psoriasis with porokeratotic eccrine ostial and dermal duct nevus. J Am Acad Dermatol 2004;50:S81-3.
[Google Scholar]
|
| 10. |
Hartman R, Rizzo C, Patel R, Kamino H, Stupak JL. Porokeratosis palmaris et plantaris disseminata or a disseminated late-onset variant of porokeratotic eccrine ostial and dermal ductal nevus (PEODDN) with follicular involvement. Dermatol Online J 2009;15:8.
[Google Scholar]
|
| 11. |
Dogra S, Jain R, Mohanty SK, Handa S. Porokeratotis eccrine ostial and dermal duct nevus: Unilateral systematized involvement. Pediatr Dermatol 2002;19:568-9.
[Google Scholar]
|
Fulltext Views
8,696
PDF downloads
2,072





![[Figure - 1]](#fig_ijdvl_2011_77_2_174_77457_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2011_77_2_174_77457_f2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2011_77_2_174_77457_f3.jpg){kind=link}