Translate this page into:
Primary cutaneous sarcomatoid carcinoma
2 Department of Pathology, College of Medicine, Soonchunhyang University, Cheonan, Korea
Correspondence Address:
Lee SungYul
Department of Dermatology, Soonchunhyang University Hospital, Bongmyung-dong, Cheonan-si, Chungnam-do
Korea
| How to cite this article: SangJin O, HanEul L, SungYul L, JongSuk L, JiHye L. Primary cutaneous sarcomatoid carcinoma. Indian J Dermatol Venereol Leprol 2012;78:665 |
Sir,
Sarcomatoid carcinoma, which rarely affects the skin and mucosal area, is regarded as a biphasic tumor composed of intimately admixed epithelial and mesenchymal malignant components. Cutaneous sarcomatoid carcinoma was first described by Edith Dawson [1] in 1972 and to date, there have been fewer than 70 reported cases, mainly in the dermatopathology literature. We herein report a very rare case of primary cutaneous sarcomatoid carcinoma on the face. Immunohistochemical and microscopic observations revealed both epithelial and mesenchymal characteristics.
An 85-year-old woman visited our department in September, 2011 with a 6-month history of solitary 2 cm × 2 cm-sized crusted erythematous mass on her face [Figure - 1]. She had no family history of similar lesions and had no previous relevant medical history, including history of local trauma or previous internal malignancy. She denied any associated pruritus or pain, but reported prior bleeding associated with trauma. Histological examination of the punch biopsy specimen taken from the lesion on the face showed irregular masses of atypical cells proliferating downward in discontiguous islands detached from the overlying epidermis; this was diagnosed squamous cell carcinoma (SCC). No regional lymph nodes were found to be enlarged on clinical examination. Chest radiograph and computed tomography scan of the neck were normal. The lesion was totally excised. On low power examination, the mass was a polypoid ulcerated and crusted tumor that measured 2 cm × 2 cm × 1 cm [Figure - 2]a. On high power view, almost scattered tumor cells were large spindle or polygonal cells having large pleomorphic nuclei with chromatin clumping and distinct nucleoli [Figure - 2]a. Mitotic activity was high (19/10 high-power fields). Atypical mitosis was also found. Only one focus of nests of typical squamous cell carcinoma is identified in the peripheral upper dermis [Figure - 2]c. There was also a transitional zone between the squamous cell carcinoma that merged into sarcomatous component. On immunohistochemical staining, the epithelial cells showed an intensive positive immunoreaction to cytokeratin 5/6 and p63. The sarcomatous cells showed a strong and diffuse expression of vimentin [Figure - 3]a, CK5/6 [Figure - 3]b, and p63 [Figure - 3]c. SMA and EMA [Figure - 3]d were focally positive. Other antibodies (CD68 and CAM5.2) were negative. After excision, whole body positron emission tomography - computed tomography (PET-CT) revealed no abnormal hypermetabolic lesions. The patient had no evidence of disease 6 months after primary excision.
 |
| Figure 1: Solitary 2 cm × 2 cm-sized crusted erythematous mass on the face |
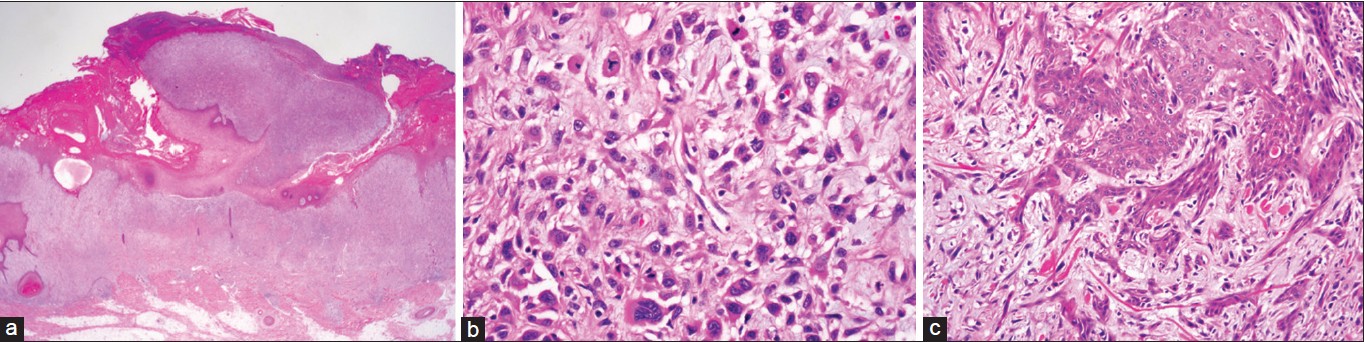 |
| Figure 2: (a) The mass is a polypoid ulcerated and crusted tumor. (H and E, ×12.5). (b) There are scattered large spindles or polygonal cells having large pleomorphic nuclei with chromatin clumping and distinct nucleoli. Mitosis is frequently seen and atypical mitosis was also found. (H and E, ×400). (c) There are sheets of typical squamous cell carcinoma. (H and E, ×400) |
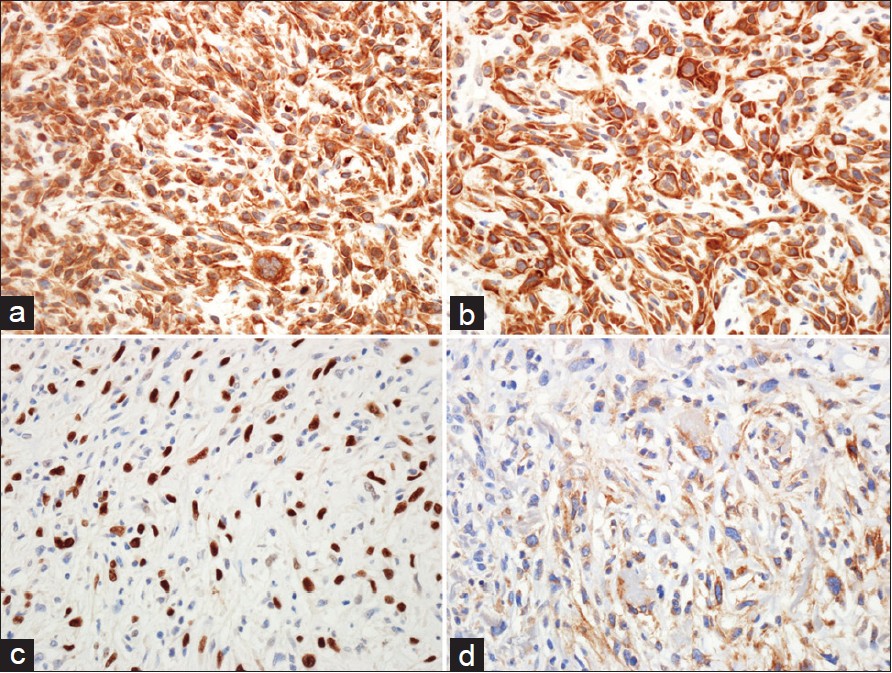 |
| Figure 3: (a) The sarcomatous cells are diffuse strong positive for vimentin (vimentin stain, ×400), (b) CK5/6 (CK5/6 stain, ×400), (c) p63 (p63 stain, ×400), (d) and focal positive for EMA. (EMA stain, ×s400) |
The coexistence of both carcinomatous and sarcomatous components in the same tumor led some authors to coin the term ′carcinosarcoma of the skin.′ This term would be plausible in the presence of a malignant epithelial component, such as BCC and SCC, in addition to a malignant mesenchymal component, such as osteosarcoma, rhabdomyosarcoma, and chondrosarcoma. Rνos-Martνn et al. [2] first coined the term sarcomatoid carcinoma of the skin after describing a unique case with features of both atypical fibroxanthoma and BCC. The histogenesis of AFX is not well-documented, but AFX has been regarded as a sarcomatoid neoplasm rather than a true sarcoma with a reasonable diagnosis. [3] The histogenesis of malignant mixed tumors remains unknown. However, two antithetic hypotheses have been suggested to explain the histogenesis of biphasic malignant tumors. The convergence hypothesis proposes an origin from two or more undifferentiated progenitor cells (multiclonal hypothesis), and the divergence hypothesis proposes an origin from a single totipotential stem cell that differentiates into separate epithelial and mesenchymal directions (monoclonal hypothesis). Presently, the most widely accepted is the divergence or monoclonal theory, which postulates that at some point, the epithelial component undergoes metaplastic transformation to lead to the malignant mesenchymal component. This may explain why patients often describe a period of recent rapid growth, suggesting that mesenchymal divergence occurs late in these cases. [4]
Surgical treatment with a 10 mm free circumferential margin including a deep excision to the fascia is recommended. There is no evidence of benefit of adjuvant chemo- or radiotherapeutic treatment on the sarcomatous part of the sarcomatoid carcinoma. Follow-up should be for at least 5 or 10 years, initially with intervals of 3-6 months. On completion of follow-up, the patient must be advised to consult a physician when there are early signs of recurrence. [5]
There is no conflicting interest, but this work was supported in part by the SoonChunHyang University Research Fund.
| 1. |
Dawson EK. Carcino-sarcoma of the skin. J R Coll Surg Edinb 1972;17:243-6.
[Google Scholar]
|
| 2. |
Ríos-Martín JJ, Parra-Martín JA, Gómez-Pascual A, Hevia-Vázquez A, González-Cámpora R. Sarcomatoid carcinoma of the skin: Report of a case. J Dermatol 1998;25:314-21.
[Google Scholar]
|
| 3. |
Rose RF, Merchant W, Stables GI, Lyon CL, Platt A. Basal cell carcinoma with a sarcomatous component (carcinosarcoma): A series of 5 cases and a review of the literature. J Am Acad Dermatol 2008;59:627-32.
[Google Scholar]
|
| 4. |
Thompson L, Chang B, Barsky SH. Monoclonal origins of malignant mixed tumors (carcinosarcomas): Evidence for a divergent histogenesis. Am J Surg Pathol 1996;20:277-85.
[Google Scholar]
|
| 5. |
Berg JO, Tei TM. Primary cutaneous carcinosarcoma: Review and presentation of a case with emphasis on clinical characteristics and management. Eur J Plast Surg 2005;28:99-104.
[Google Scholar]
|
Fulltext Views
4,039
PDF downloads
2,565





![[Figure - 1]](#fig_ijdvl_2012_78_5_665_100536_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2012_78_5_665_100536_f2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2012_78_5_665_100536_f3.jpg){kind=link}