Translate this page into:
Pseudoepitheliomatous, keratotic, and micaceous balanitis presenting as cutaneous horn in an adult male
2 Department of Pathology, SDM College of Medical Sciences and Hospital, Dharwad - 580 009, Karnataka, India
Correspondence Address:
Varadraj V Pai
Department of Dermatology, SDM College of Medical Sciences, Dharwad - 580 009, Karnataka
India
| How to cite this article: Pai VV, Hanumanthayya K, Naveen K N, Rao R, Dinesh U. Pseudoepitheliomatous, keratotic, and micaceous balanitis presenting as cutaneous horn in an adult male. Indian J Dermatol Venereol Leprol 2010;76:547-549 |
Abstract
Pseudoepitheliomatous, keratotic, and micaceous balanitis is an extremely rare condition occurring over the glans in elderly characterized by silvery white plaque with mica-like crust, which can undergo malignant transformation. Herein we present a case of pseudoepitheliomatous, keratotic, and micaceous balanitis occurring in an adult male presenting as a cutaneous horn.Introduction
Pseudoepitheliomatous, keratotic, and micaceous balanitis is an extremely rare condition occurring over the glans in the elderly and characterized by silvery white plaque with mica-like crust. [1] Ulcerations, cracking, and fissuring have been noted in a few instances. In some cases, the condition may progress to verrucous carcinoma or squamous cell carcinoma. Herein we report for the first time a case of "Pseudoepitheliomatous, keratotic, and micaceous balanitis presenting as cutaneous horn in an adult male."
Case Report
A 35-year-old male presented to our dermatology out-patient department (OPD) with history of lesion over the penis of 5 months duration. The lesion was not visible due to preexisting phimosis for which he had circumcision 2 months back. The lesion, now visible, was asymptomatic and increasing in size. There was no history of exposure to sexually transmitted infections, diabetes, or urethral symptoms. The patient gave a history of topical application of antiseptic and keratolytic creams.
Examination revealed a circumcised penis with two irregular plaques over the glans penis, the larger plaque measuring 1.5 Χ 1.0 cm showed a central cutaneous horn (0.7Χ0.7 cm) with mild crusting and peripheral scaling. The smaller plaque measuring 0.5Χ 0.5 cm also showed central crusting and peripheral scaling. Both lesions were firm and nontender [Figure - 1]. There was no inguinal lymphadenopathy.
 |
| Figure 1 :Central cutaneous horn surrounded by crusts and scaling at the margins |
Blood counts and blood glucose were within normal limits. Tests for HIV antibodies and hepatitis B surface antigen were negative and the VDRL test was nonreactive. Incision biopsy of larger plaque revealed features of hyperkeratosis, acanthosis, parakeratosis, elongation of rete ridges, and mild lower epidermal dysplasia with eosinophils and lymphocytes in a non-specific dermal inflammatory cell infiltrate [Figure - 2].
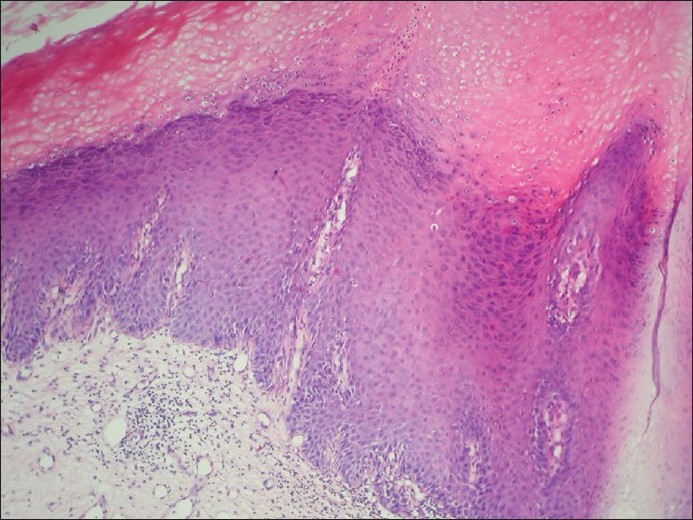 |
| Figure 2 :Hyperkeratosis, parakeratosis, elongation of rete ridges and mild lower epidermal dysplasia with eosinophils and lymphocytes in a non-specific dermal inflammatory cell infiltrate (H and E, ×40) |
A diagnosis of pseudoepitheliomatous, keratotic, and micaceous balanitis of Civatte was made. The patient was started on topical 5-flourouracil and was followed up only once without much improvement and later lost to follow up.
Discussion
In 1961 Lortat-Jacob and Civatte [2] described the first case of pseudoepitheliomatous, keratotic, and micaceous balanitis in the French literature. The lesion described by them presented as thick, hyperkeratotic plaques that spread locally. Later on cases were described in the English literature and till date there are less than 20 cases in the English literature.
It is mainly seen in the elderly (over 60 years), [3],[4],[5] unlike our patient who presented at a younger age. Similar to the first reported case our patient too had pre-existing phimosis. [2] The exact etiology is not known. Originally the lesion was thought to be benign or of limited malignant potential, [2],[3] but in 1987 Beljaards, van Dijk, and Hausman reported two cases of "pseudoepitheliomatous, keratotic, and micaceous balanitis," both of which progressed to verrucous carcinoma with subsequent development of invasive squamous cell carcinoma in one case. [4]
The pathogenesis of PKMB occurs in four stages: (a) initial plaque stage, (b) late tumor stage, (c) verrucous carcinoma, and (d) transformation to squamous cell carcinoma and invasion. [5]
Clinically, the plaque stage begins as coronal balanitis, gradually develops a silvery white appearance, and subsequently mica-like crusts and keratotic masses form on the glans. In our patient the primary lesion was unnoticed because of the pre-existing phimosis. Out of the 15 cases described in the English literature, 6 progressed to verrucous carcinoma, 4 cases developed squamous cell carcinoma (SCC), out of which 2 had progressed from verrucous carcinoma to invasive squamous cell carcinoma. [6]
The differential diagnosis includes squamous cell carcinoma, verrucous carcinoma, keratoacanthoma, giant condyloma, penile horn, and erythroplasia of Queyrat. [7]
Treatment is based on the stage of the lesion, with the initial plaque stage requiring topical therapy and the advanced stages necessitating more aggressive therapy. Treatment includes topical 5-flourouracil and cryotherapy, when there is no histological evidence of malignancy. [5] Extensive surgical excision is required in cases having features of atypia with good cosmetic and functional results. [7]
This case is being reported in view of the rarity of "pseudoepitheliomatous, keratotic, and micaceous balanitis," the need for early diagnosis and long term follow-up in view of the potential for malignant transformation.
| 1. |
Subudhi CL, Singh PC. Pseudoepitheliomatous, keratotic and micaceous balanitis producing nail-like lesion on the glans penis. Indian J Dermatol Venereol Leprol 1999;65:75-7.
[Google Scholar]
|
| 2. |
Lortat-Jacob E, Civatte J. Balanite pseudoepitheliomateuse, kertosique micacee. Bull Soc Fr Dermatol Syphiligr 1961;68:164-7.
[Google Scholar]
|
| 3. |
Bart RS, Kopf AW. On a dilemma of penile horns: pseudoepitheliomatous, hyperkeratotic and micaceous balanitis? J Dermatol Surg Oncol 1977;3:580-2.
[Google Scholar]
|
| 4. |
Beljaards RC, Van Dijk E, Hausman R. Is pseudoepitheliomatous, micaceous, and keratotic balanitis synonymous with verrucous carcinoma? Br J Dermatol 1987;117:641-6.
[Google Scholar]
|
| 5. |
Krunic AL, Djerdj K, Starcevic-Bozovic A, Kozomara MM, Martinovic NM, Vesic SA, et al. Pseudoepitheliomatous, keratotic, and micaceous balanitis. Urol Int 1996;56:125-8.
[Google Scholar]
|
| 6. |
Perry D, Lynch PJ, Fazel N. Pseudoepitheliomatous, keratotic, and micaceous balanitis: Case report and review of the literature. Dermatol Nurs 2008;20:117-20.
[Google Scholar]
|
| 7. |
Reed SI, Abell E. Pseudoepitheliomatous, keratotic and micaceous balanitis. Arch Dermatol 1981;117:435-7.
[Google Scholar]
|
Fulltext Views
7,499
PDF downloads
1,782





![[Figure - 1]](#fig_ijdvl_2010_76_5_547_69087_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2010_76_5_547_69087_f2.jpg){kind=link}