Translate this page into:
Psoriasiform skin eruption associated with sorafenib therapy
2 Department of Pathology, Hospital Universitario Marqu�s de Valdecilla, Universidad de Cantabria, Santander, Spain
Correspondence Address:
Marcos A Gonz�lez-L�pez
Hospital Universitario Marqu�s de Valdecilla, Avda. Valdecilla s/n, E-39008 Santander
Spain
| How to cite this article: Gonz�lez-L�pez MA, Gonz�lez-Vela M C, Y��ez S, Fern�ndez-Llaca H, Val-Bernal J F. Psoriasiform skin eruption associated with sorafenib therapy. Indian J Dermatol Venereol Leprol 2011;77:614-615 |
Sir,
Sorafenib is an oral multi-targeted kinase inhibitor with anti-angiogenic and anti-proliferative activity. [1] It is approved for treatment of unresectable hepatocellular carcinoma and advanced renal carcinoma. Sorafenib acts by inhibition of several receptor tyrosine kinases, such as vascular endothelial growth factor receptor (VEGFR), platelet-derived growth factor receptor (PDGFR), c-kit and the intracellular Raf kinase (Raf-1). [1] Cutaneous toxicity is relatively common in patients receiving sorafenib. The most frequent cutaneous side effect is the hand-foot syndrome; other described adverse skin reactions include facial erythema, acral erythema, erythema multiforme, subungual splinter hemorrhage, stomatitis, and alopecia. [1] Recently, two cases of sorafenib-associated psoriasiform eruption have been reported. [1],[2] Furthermore, exacerbation of psoriasis was also described after treatment with the EGFR tyrosine kinase inhibitor gefitinib. [3] Moreover, a case of psoriasiform plaques histopathologically suggestive of acute generalized exantematous pustulosis have also been reported with lapatinib, another multikinase inhibitor. [4] We present herein an additional case of a patient who developed cutaneous psoriatic lesions following sorafenib therapy.
A 59-year-old man was diagnosed of nodular hepatocellular carcinoma secondary to alcoholic liver cirrhosis in July 2009. The tumor was surgically excised. In November 2009, multiple lung metastases were detected bilaterally on chest CT scan. Sorafenib 400 mg orally twice daily was then initiated with a good clinical response. In March 2010, 4 months later, he developed an extensive cutaneous eruption involving the trunk and limbs. The patient had no personal or family history of psoriasis, and he was not receiving simultaneously any other medication. Dermatological examination revealed multiple erythematous, scaly, papules and plaques on the thorax, abdomen, back, and proximal areas of the limbs. The psoriasiform lesions were mainly of guttate type and showed Koebner΄s phenomenon [Figure - 1]. A skin biopsy specimen disclosed psoriasiform hyperplasia of the epidermis with confluent parakeratosis and dilated vessels in the papillary dermis, consistent with psoriasiform eruption [Figure - 2]. Despite this side effect, sorafenib therapy was continued because the drug was effective in the control of the metastatic progression. The cutaneous lesions improved significantly after treatment with topical steroids and narrow-band UVB phototherapy.
 |
| Figure 1: Multiple psoriasiform lesions mainly of the guttate type on the trunk that show Koebner´s phenomenon |
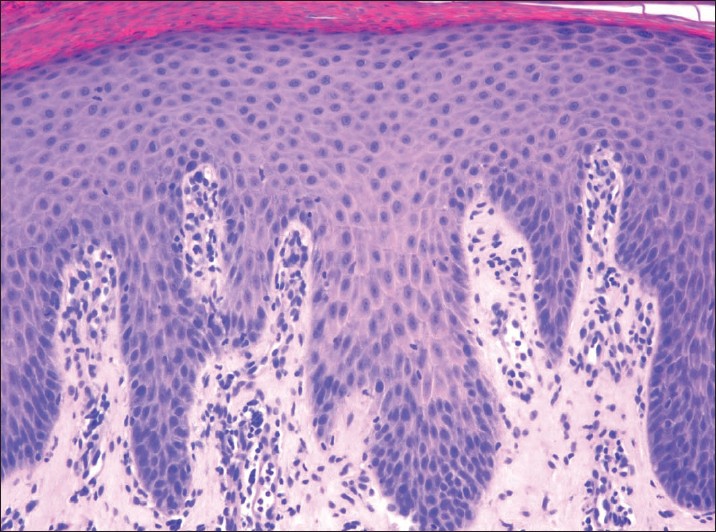 |
| Figure 2: The epidermis showed a psoriasiform hyperplasia with confluent parakeratosis. (H and E, ×100) |
The development of psoriasiform eruptions in patients treated with sorafenib seems paradoxical, since this drug blocks the activity of VEGF, a cytokine whose role in psoriasis pathogenesis is well documented. Thus, it has been reported an overexpression of VEGF on psoriatic keratinocytes and upregulation of VEGF receptors in microvasculature of psoriatic lesions. [5] Furthermore, elevated levels of VEGF can be detected in the serum of human psoriasis patients and correlates with disease activity. [6] On this basis, drugs against VEGF or its receptor are being considered as future therapies for psoriasis. [5] To this respect, a patient with metastatic hypernephroma treated with sorafenib was associated with remission of his recalcitrant psoriatic lesions. [7] However, in our patient the implication of this drug in the development of the psoriasiform eruption seems likely given that: (a) there was no previous history of psoriasis, and he had not taken any drug known to be associated with psoriasiform eruptions, and (b) the temporal relationship between the initiation of sorafenib and the onset of skin disorder.
The pathogenesis of sorafenib-induced psoriasiform eruptions is difficult to explain. Nevertheless, it should be noted that other cutaneous disorders characterized by epidermis proliferation, such as palmar-plantar hyperkeratosis and keratoancanthomas have been described in patients on sorafenib therapy. [1],[8] This suggest that sorafenib might alter the keratinocyte proliferation and differentiation by a yet unknown mechanism. Future investigations may increase our understanding of this.
In summary, sorafenib should be added to the list of drugs that can potentially cause a psoriasiform eruption.
| 1. |
Diamantis ML, Chon SY. Sorafenib-induced psoriasiform eruption in a patient with metastatic thyroid carcinoma. J Drugs Dermatol 2010;9:169-71.
[Google Scholar]
|
| 2. |
Laquet V, Saedi N, Dann F, Kelly K. Sorafenib-associated psoriasiform skin changes. Cutis 2010;85:301-2.
[Google Scholar]
|
| 3. |
Zorzou MP, Stratigos A, Efstathiou E, Bamias A. Exacerbation of psoriasis after treatment with an EGFR tyrosine kinase inhibitor. Acta Derm Venereol 2004;84:308-9.
[Google Scholar]
|
| 4. |
Lakshmi C, Pillai SB, Srinivas CR. Lapatinib-induced acute generalized exanthematous pustulosis. Indian Dermatol Online J 2010;1:14-7.
[Google Scholar]
|
| 5. |
Halin C, Fahmgruber H, Meingassner JG, Bold G, Littlewood-Evans A, Stuetz A, et al. Inhibition of chronic and acute skin inflammation by treatment with a vascular endothelial growth factor receptor tyrosine kinase inhibitor. Am J Pathol 2008;173:265-77.
[Google Scholar]
|
| 6. |
Nofal A, Al Makhzangy I, Attwa E, Nassar A, Abdalmoati A. Vascular endothelial growth factor in psoriasis: An indicator of disease severity and control. J Eur Acad Dermatol Venereol 2009;23:803-6.
[Google Scholar]
|
| 7. |
Fournier C, Tisman G. Sorafenib-associated remission of psoriasis in hypernephroma: Case report. Dermatol Online J 2010;16:2.
[Google Scholar]
|
| 8. |
M, Jacobson M, Burges GE, Dewaay D, Maize JC Jr, Chaudhary UB. Localized palmar-plantar epidermal hyperplasia: A previously undefined dermatologic toxicity to sorafenib. Oncologist 2007;12:178-82.
[Google Scholar]
|
Fulltext Views
3,847
PDF downloads
2,495





![[Figure - 1]](#fig_ijdvl_2011_77_5_614_84089_u1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2011_77_5_614_84089_u2.jpg){kind=link}