
Translate this page into:
Rapid onset acquired progressive kinking of the hair: Scanning electron microscopic findings in a woman
Corresponding author: Dr. Gulsen Tukenmez Demirci, Acıbadem Altunizade Hastanesi, Tophanelioğlu Cad., Yurtcan Sok., No. 1, Altunizade Üsküdar 34662, İstanbul, Turkey. gulsentukenmez@yahoo.com
-
Received: ,
Accepted: ,
How to cite this article: Civas E, Demirci GT. Rapid onset acquired progressive kinking of the hair: Scanning electron microscopic findings in a woman. Indian J Dermatol Venereol Leprol 2021;87:281-4.
Acquired progressive kinking of the hair is a rare hair shaft disorder and we found less than 30 previously reported cases in the literature. The etiology of acquired progressive kinking of the hair is still unknown. It has been proposed as a possible mechanism wherein kinking of the hair is a hair cycle disorder related to the shortening of anagen hairs and dysregulation in the inner root sheath of the hair bulb.1
A 44-year-old woman presented to our clinic with a complaint of stagnation of hair growth with an unruly, coarse and dull appearance for the last 3 years. She had received a keratin treatment at a hairdresser 3 weeks before the symptoms started.
On dermatological examination, there was a slight regression of the frontal hairline, along with kinky hairs distributed diffusely, more prominently seen over the parietal and frontal areas of the scalp. The kinky hairs were located mostly 4–5 cm apart from the proximal of the frontal hairline and 6–7 cm apart from the proximal of parietal and vertex hairs and less prominent on occipital hairs [Figures 1a, b and c].

- Diffuse kinking of the hairs

- The kinking hairs on parietal and vertex area

- The kinking hairs seen prominently on frontal area
Her systemic examination was normal. She has been using cyproterone acetate 2 mg/ethinyl estradiol 0.035 mg for polycystic ovary syndrome over the last 15 years. Her complete blood counts, liver and kidney function tests, serum ferritin, vitamin D, thyroid-stimulating hormone, free thyroxine, biotin, zinc, copper, vitamin B12, follicle stimulating hormone and luteinizing hormone, estradiol, total and free testosterone, prolactin and dehydroepiandrosterone- sulfate levels were normal.
Trichogram findings comprised 81.1% anagen and 18.9% telogen hairs along with 97% terminal and 3% vellus hairs. (parameters were measured by FotoFinder Trichoscale Professional program) [Figure 2a].
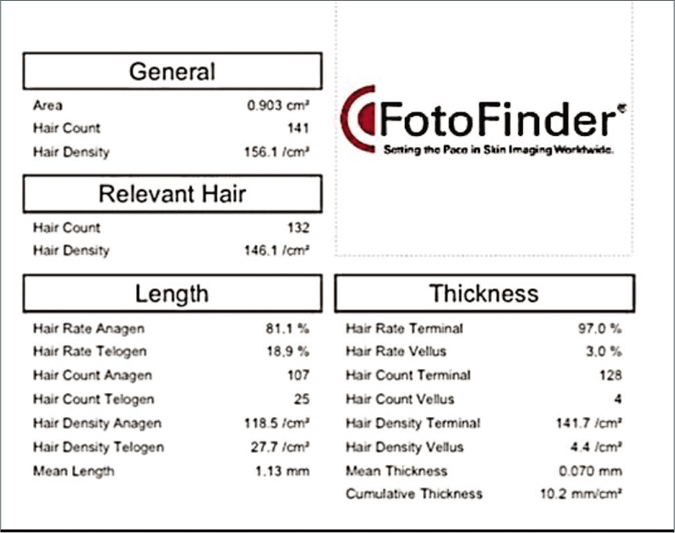
- Trichogram findings of the patient. (FotoFinder Trichosscale
We observed that hair count, hair diameter, distribution of hair in the hair unit were within normal limits after trichoscopic examination. There were some hairs with interrupted medulla over parietal areas [Figure 2b]. Mild scaling was seen over the scalp.
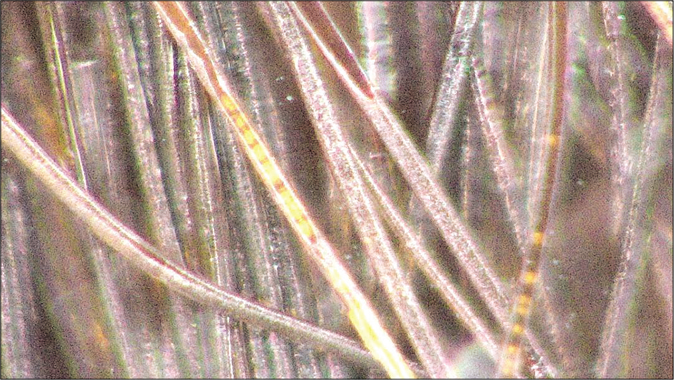
- The tricoscopic image of the interrupted medulla finding of the hair shaft. (FotoFinder Medicam, polarized Light, ×700)
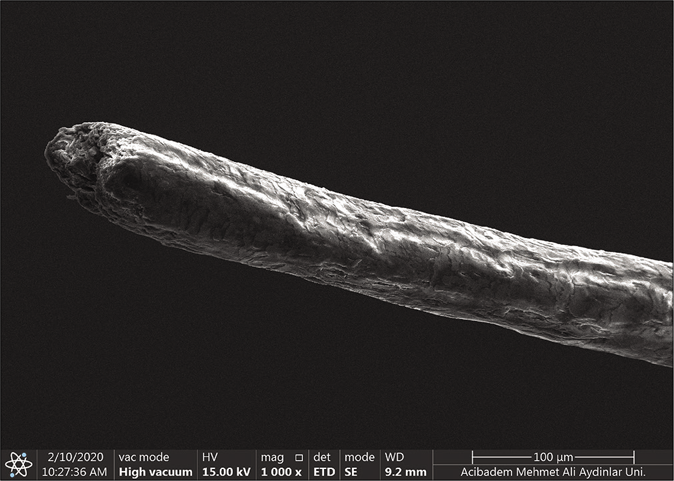
Scanning electron microscopy analysis (Thermo scientific Quattro, Czech Republic Vlastimila Pecha 1282/12) showed partial bending and twisting of hair on its longitudinal axis, pili canaliculi, transverse splitting of hair and damaged cuticular cells in twisted hairs. Trichorrhexis nodosa in some hairs and thinning of the diameter in the distal parts of the hair were also evident [Figure 3].
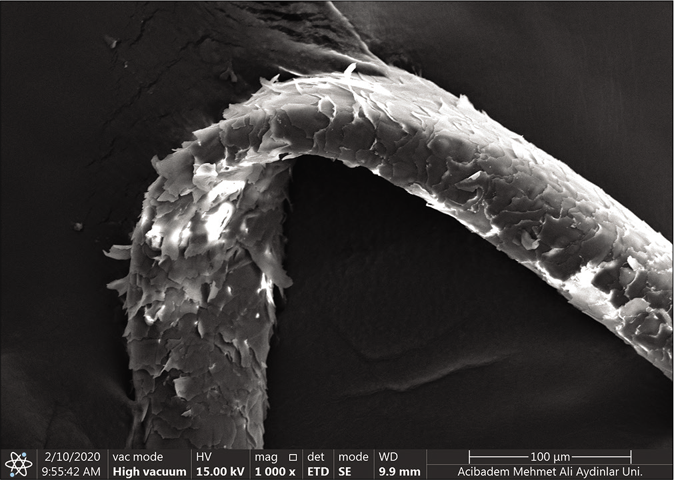
- Scanning electron microscopic (Thermo Scientific Quattro, Czech Republic Vlastimila Pecha 1282/12) findings of the patient. Bending of the hair shaft on its long axis and the raised cuticle (×1000)
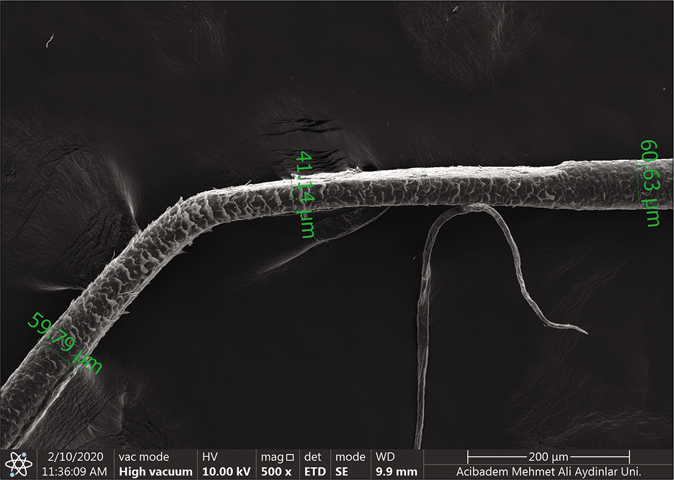
- Scanning electron microscopic (Thermo Scientific Quattro, Czech Republic Vlastimila Pecha 1282/12) findings of the patient. Bending of the hair shaft, a sharp reduction in hair diameter (×500)
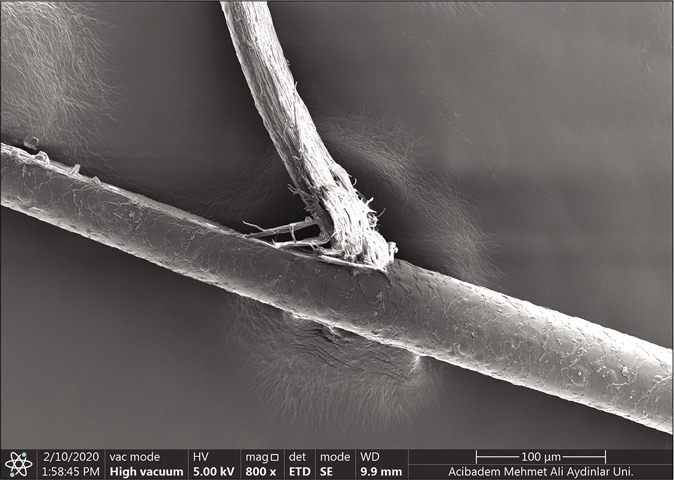
- Scanning electron microscopic (Thermo Scientific Quattro, Czech Republic Vlastimila Pecha 1282/12) findings of the patient. The transverse splitting of the hair shaft (×800)
- Scanning electron microscopic (Thermo Scientific Quattro, Czech Republic Vlastimila Pecha 1282/12) findings of the patient. Pili canaliculi, the canal formation on the hair shaft (×1200)
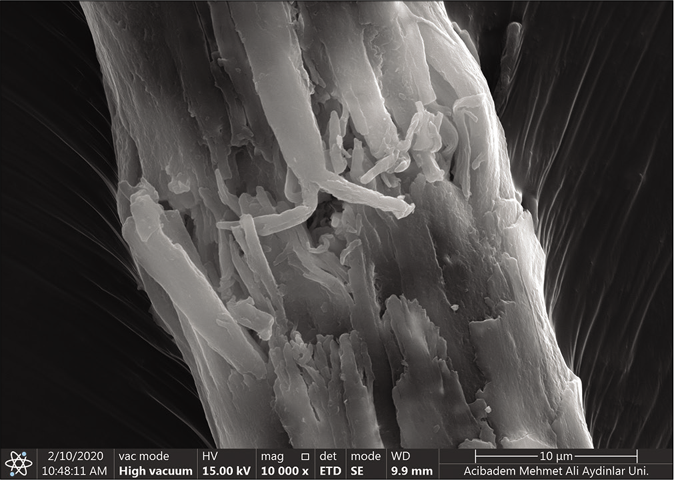
- Scanning electron microscopic (Thermo Scientific Quattro, Czech Republic Vlastimila Pecha 1282/12) findings of the patient. Trichorrhexis nodosa (×10,000)
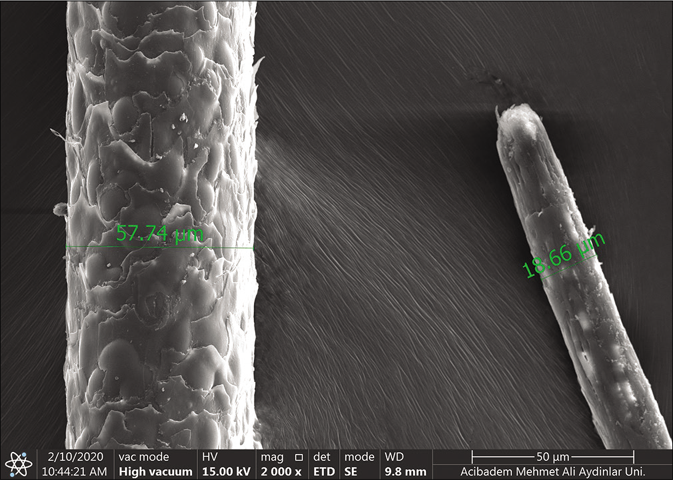
- Scanning electron microscopic (Thermo Scientific Quattro, Czech Republic Vlastimila Pecha 1282/12) findings of the patient. Measurement of the proximal diameter (57.74 μm) and the distal diameter of the same hair shaft (18.66 μm) (×2000)
Balsa et al. defined the diagnostic method for acquired progressive kinking of the hair in 1986 as follows: (1) An acquired circumscribed area of dull, woolly hair in the frontal, temporal or parietal region in the absence of previous trauma. Irregular, twisted and tortuous hair with the first twist appearing at 3–4 cm from the emergence of the hair. (2) On optical microscopy, a periodic reduction in the hair shaft diameter with broadened sections alternating with flattened ones. (3) On scanning electron microscopy, a partial twisting of the hair on its longitudinal axis with a 180-degree rotation, variable pili canaliculi (or longitudinal grooves), spindle-shaped broadening with occasional fractures and increased number of cuticular cells per diameter in the twisted sections.1 Our case fulfilled the criteria of Balsa et al.
Moreover, in scanning electron microscopy examination, we observed transverse splitting, trichorrhexis nodosa and increased cuticular cells in some hair shafts which could be related to the physical trauma caused by hairdryers.
Acquired progressive kinking of the hair was classified into five types according to the cases reported in the literature by Tosti et al. in 1999. They reported some cases in women and prepubertal cases which were not related to androgenetic alopecia. In two cases of type 3, patients were diagnosed with rapid onset and progressive kinking of hair similar to our case. One of them had a history of permanent hair wave procedure before the onset of the disorder.2 Osorio and Tosti stated that traumatic and chemical cosmetic procedures may disrupt the hair shaft but as the hair is a nonliving structure, acquired damage to the hair shaft is irreversible; however, hair is in continuous growth and can be restored.3 In our case, keratin treatment of hair could not be accepted as a definitive cause since the progression of the disorder was around 3 years.
There have been some reports of acquired progressive kinking of the hair cases that were found to be related to some drugs like acitretin, etretinate, ribavirin, interferon and chemotherapeutics.4 In the present case, our patient was taking cyproterone acetate 2 mg, plus ethinylestradiol 0.035 mg for 15 years. Cyproterone can directly block androgen receptors and decrease testosterone levels, therefore, it can improve hair growth in androgenetic alopecia in females.5 In our patient, the trichogram showed early stages of androgenetic alopecia. We considered that the cyproterone acetate/ethinylestradiol may have suppressed the formation of androgenetic alopecia. In conclusion, the rapid onset of this hair disorder may be due to a previous hair cosmetic procedure but the progression of the disorder may be caused by masked androgenetic alopecia.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Acquired kinking of the hair: A methodologic approach. J Am Acad Dermatol. 1986;15:1133-6.
- [CrossRef] [Google Scholar]
- Acquired progressive kinking of the hair: Clinical features, pathological study, and follow-up of 7 patients. Arch Dermatol. 1999;135:1223-6.
- [CrossRef] [Google Scholar]
- Hair Weathering, part 1: Hair structure and pathogenesis. J Cosmet Dermatol. 2011;24:533-34.
- [Google Scholar]
- Acquired progressive kinking of the hair in an elderly woman: A case report. Dermatol Online J 2018:15-24.
- [Google Scholar]
- Antiandrogenic therapy with ciproterone acetate in female patients who suffer from both androgenetic alopecia and acne vulgaris. Clujul Med. 2014;87:226-34.
- [CrossRef] [PubMed] [Google Scholar]




