Translate this page into:
Removal of corns by punch incision: A retrospective analysis of 15 patients
Correspondence Address:
Şule G�ng�r
Dar�llacize Street, Okmeydanı Hospital, Şişli, Istanbul 34000
Turkey
| How to cite this article: G�ng�r &, Bah�etepe N, Topal &. Removal of corns by punch incision: A retrospective analysis of 15 patients. Indian J Dermatol Venereol Leprol 2014;80:41-43 |
Abstract
Background: Hard corns are firm, small, dome-shaped papules with translucent central cores, which occur on the palmoplantar region of toes and hands due to repeated trauma. Medical management of hard corns is difficult and sometimes requires surgical excision. Punch incision is a technique which is performed using a circular blade or trephine attached to a pencil-like handle. Aim: We hypothesized that it might serve as an alternative method to surgical excision in the treatment of recalcitrant corns and performed the technique to treat 17 corns in 15 patients. The present study aimed to review these 15 patients retrospectively and evaluate the effectiveness of punch incision. Method: A total of 15 patients with recalcitrant corns were treated using punch incision between April 2011 and December 2012 and were evaluated by photographs and patient satisfaction questionnaires. Results: Out of the 17 corns, 3 corns persisted after punch incision and the patients were referred to the orthopedic clinic for further treatment; 2 of the 17 corns partially responded and required additional topical treatment; and 12 of the 17 corns responded completely to punch incision. Conclusion: Punch incision is a simple and effective technique for the treatment of small corns on the palms and soles.Introduction
Hard corns are firm, small, dome-shaped papules with translucent central cores that occur on the palmoplantar region of toes and hands due to repeated trauma. [1] Calluses are broad-based, superficial lesions and medical management is more successful; whereas corns are narrow-based, sharply defined and deep lesions, so medical management is difficult and sometimes surgical excision is required. [1]
Punch incision is a technique performed using a circular blade or trephine 2-6 mm in diameter and 1 cm in length, attached to a pencil-like handle. [2] The advantages of this technique versus classical elliptical excision are that it facilitates obtaining deeper and narrower tissue, causes less damage to peripheral tissue, is associated with more rapid healing and less scarring and is simpler and easier to perform. [3]
Previously, punch incision had been introduced as an alternative method for surgical excision of epidermal inclusion cysts, trichilemmal cysts, and sebaceous cysts. [3],[4] Based on the current knowledge of punch incision, we hypothesized that it might serve as an alternative method to surgical excision in the treatment of recalcitrant corns and performed the technique to treat 17 corns in 15 patients.
The present study aimed to review these 15 patients retrospectively and evaluate the effectiveness of punch incision.
Methods
Informed consent was obtained from all patients prior to enrollment. The study protocol conformed to the guidelines of the 1975 Declaration of Helsinki.
Seventeen recalcitrant corns of 15 patients were treated using punch incision between April 2011 and December 2012 and were evaluated using photographs and patient satisfaction questionnaires. None of the patients had any systemic or vascular disease.
Photographic evaluation was performed by 2 independent dermatologists comparing pre-treatment and post-treatment photographs. Patient satisfaction was evaluated during the follow-up visits; based on the relief or not.
Punch incision technique
Following adequate skin preparation, we achieved local anesthesia through injection of 1% lidocaine into the peripheral tissue only, not into the corn. A single-use disposable 3-6-mm punch biopsy instrument was held vertically over the skin and rotated downward using a twirling motion. After the instrument penetrated the dermis into the subcutaneous fat, or after the instrument reached the hub, it was removed [Figure - 1]. Hemostasis was achieved, and then the wound was left to heal through secondary intention. Antiseptic ointment was applied to the wound 3 times a day for 2 weeks. Five of the removed tissue sample were examined histopathologically to confirm the diagnosis.
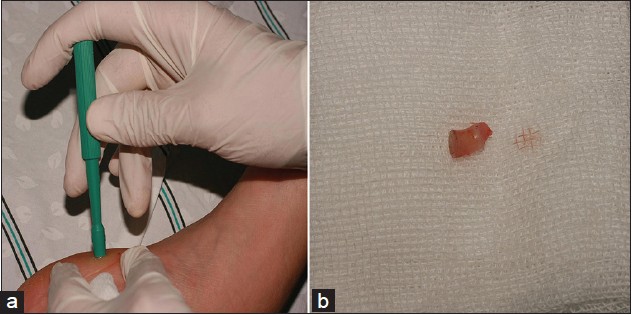 |
| Figure 1: (a) A single-use disposable 3-6-mm punch biopsy instrument was held vertically over the skin and rotated downward using a twirling motion, (b) Removed tissue |
Results
Three men and 12 women were included in the study. Patients′ ages ranged from 24 to 55 years. Lesion duration varied from 1 year to 7 years; lesion size varied from 3 mm to 7 mm. One lesion was located on the palm, the other lesions were located on the soles.
Out of the 17 recalcitrant corns, 3 persisted after punch incision and the patients were referred to the orthopedic clinic for further treatment. In 2 of the 17 corns partial pain relief was achieved 4 weeks after punch incision, and an ointment containing salicylic acid and urea was applied to these areas leading to complete relief in 4 weeks. After 6 months, one corn recurred. In 10 of the 15 patients (12 of the 17 corns) total pain relief was achieved 4 weeks after punch incision without any recurrence during 6 months of follow-up [Figure - 2]. Overall, 13 of 17 corns were clear on photographs after 6 months of follow-up.
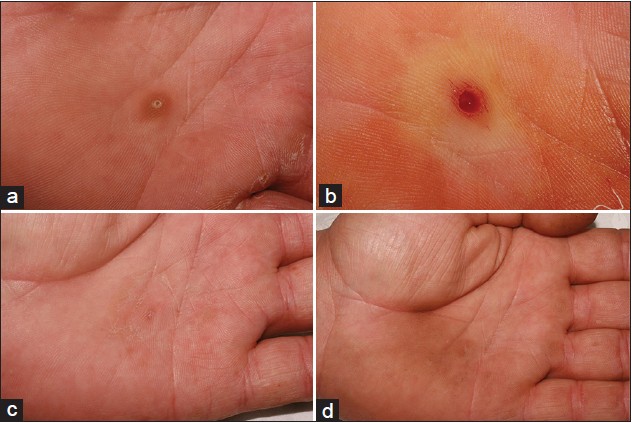 |
| Figure 2: (a) Corn on the palmar side of the hand, (b) Immediately after punch incision (PI), (c) 6 weeks after PI, (d) 6 months after PI |
Minor pain was reported by the patients during local anesthesia. Minor bleeding occurred immediately after incision in all cases and the incisions healed with a crust within a few weeks. No other side-effects were noted during treatment or the post-treatment period.
Dicussion
Corns and calluses are hyperkeratotic tissues that result from repeated trauma and pressure. In particular, corns are very painful because they are sharp and deep. In general, medical management such as keratolytics is sufficient for the treatment of calluses, but not corns. There is a hard, translucent whitish-yellow core at the center of corns that must be removed mechanically to provide prompt relief. When medical management fails, surgical excision is performed. We hypothesized that the punch incision technique would be more effective for the treatment of corns than classical elliptical excision as punch incision is associated with more rapid healing and less bleeding in addition to the fact that the procedure is quicker and easier to perform.
In the present study, 3 of the 15 patients did not have pain relief after punch incision, this may be because the punch diameter was smaller than the corn diameter in these cases. As the treatment was experimental and we had no prior experience in treating corns with punch incision, we thought that use of a punch biopsy instrument smaller than the corn would be sufficient but the outcome in these cases clearly indicated that the corn must be completely removed. One of the non - responsive corns was of long duration (7 years) and large (7 mm), both of which may have led to treatment failure. Twelve of the 17 corns completely responded to punch incision. The size of the corns that responded completely varied from 3 mm to 5 mm and their duration varied from 1 year to 3 years. Punch diameters were the same or 1 mm larger than corn diameter in these cases and this may explain the high rate of treatment response.
Sacchidanand et al. described this technique for treating corns and reported their experience in six patients; [5] however, they did not use local anesthesia before incision, as was performed in the present study. In the present study local anesthetic was injected into the periphery of the corn but not into the corn as it is too hard for injection of a liquid and unnecessary because it is not sensitive to pain. Punch incision was performed in the first three patients without local anesthesia and punch tools smaller than the corns were used in an effort to protect the peripheral tissue, but the treatment failed. The following patients received local anesthetic injected into the peripheral tissue and we used punch tools that were the same size or larger than the corns, excising not only keratinous tissue but also some normal tissue, which proved to be more effective. Therefore, we recommend the use of a punch tool that is the same size or larger than the corn.
Conclusion
Based on the above study it can be concluded that punch incision is a simple and effective technique for the treatment of small corns on the palms and soles.
| 1. |
Smith ML. Environmental and sports-related skin diseases. In: Bolognia JL, Jorizzo JL, Rapini RP editors. Dermatology. 2 nd ed. Spain: Mosby Elsevier; 2008. p. 1367.
[Google Scholar]
|
| 2. |
Zuber TJ. Punch biopsy of the skin. Am Fam Physician 2002;65:1155-8, 1161.
[Google Scholar]
|
| 3. |
Mehrabi D, Leonhardt JM, Brodell RT. Removal of keratinous and pilar cysts with the punch incision technique: Analysis of surgical outcomes. Dermatol Surg 2002;28:673-7.
[Google Scholar]
|
| 4. |
Lee HE, Yang CH, Chen CH, Hong HS, Kuan YZ. Comparison of the surgical outcomes of punch incision and elliptical excision in treating epidermal inclusion cysts: A prospective, randomized study. Dermatol Surg 2006;32:520-5.
[Google Scholar]
|
| 5. |
Sacchidanand S, Mallikarjuna M, Purohit V, Sujaya SN. Surgical enucleation of corn: A novel technique. J Cutan Aesthet Surg 2012;5:52-3.
[Google Scholar]
|
Fulltext Views
10,911
PDF downloads
3,698





![[Figure - 1]](#fig_ijdvl_2014_80_1_41_125491_f1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2014_80_1_41_125491_f2.jpg){kind=link}