Translate this page into:
Response of superimposed linear psoriasis to ustekinumab: A case report
Corresponding Author:
Tsen-Fang Tsai
Department of Dermatology, National Taiwan University Hospital, 7 Chung-Shan South Road, Taipei 10048
Taiwan
tftsai@yahoo.com
| How to cite this article: Weng HJ, Tsai TF. Response of superimposed linear psoriasis to ustekinumab: A case report. Indian J Dermatol Venereol Leprol 2017;83:392-396 |
Sir,
Linear psoriasis is a rare form of psoriasis which has been reported to concur with plaque psoriasis but may be unmasked only after the effective treatment of plaque psoriasis on other body parts.[1],[2] Most of the literature till now demonstrated that treatments effective for plaque psoriasis including adalimumab, infliximab, etanercept, methotrexate, dithranol and corticosteroids, only yielded poor to limited responses in linear psoriasis.[1],[2],[3],[4] There is only one report in which radiation therapy combined with calcipotriol and corticosteroids was somewhat effective.[5]
Here we present a case in which linear psoriasis showed inadequate response to ustekinumab, an anti-interleukin-23 monoclonal antibody. A 26-year-old otherwise healthy man was diagnosed with plaque psoriasis, two years before his visit at our clinic. His previous regimen included oral methotrexate, oral acitretin, topical calcipotriol, topical calcitriol and topical clobetasol propionate. Nevertheless, the skin lesions continued to increase. At the age of 27, he noticed linear lesions developing on his right arm. On physical examination, he had multiple individual erythematous scaly plaques coalescing to form a linear pattern on his right upper arm, shoulder and back [Figure 1a] and [Figure 1b] along with typical plaque psoriasis [Figure 1c]. Due to intolerance to other treatments, ustekinumab 45 mg was administered subcutaneously at weeks 0 and 4, followed by every 4 weeks. Over the treatment course of 18 doses, most lesions of plaque psoriasis showed a significant resolution, with psoriasis area and severity index (PASI) dropping from 14.3 to 3.2. However, linear psoriasis on the arm and back remained refractory to ustekinumab and was especially pruritic [Figure 2a],[Figure 2b],[Figure 2c]. Biopsies on the lesions from linear and plaque psoriasis were both compatible with the diagnoses of psoriasis. Acanthosis, elongation of rete ridges, hyperkeratosis, Munro's microabscesses and upper dermal lymphocytic and neutrophilic infiltration were observed in both lesions [Figure 3a] and [Figure 3b].
 |
| Figure 1a: Before the initiation of ustekinumab: Superimposed linear psoriasis on the back |
 |
| Figure 1b: Before the initiation of ustekinumab: Superimposed linear psoriasis on the right arm |
 |
| Figure 1c: Before the initiation of ustekinumab: Plaque psoriasis on the leg |
 |
| Figure 2a: Refractory lesions of linear psoriasis after ustekinumab: Persistent lesions of linear psoriasis on the back |
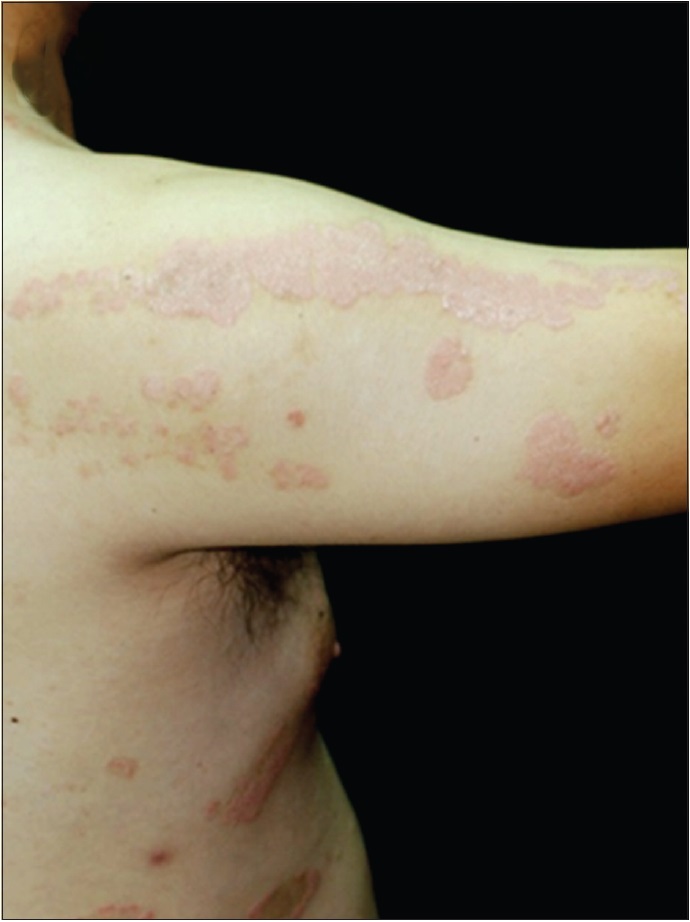 |
| Figure 2b: Refractory lesions of linear psoriasis after ustekinumab: Persistent lesions of linear psoriasis on the right arm |
 |
| Figure 2c: Lesions of plaque psoriasis over the legs showing improvement after ustekinumab |
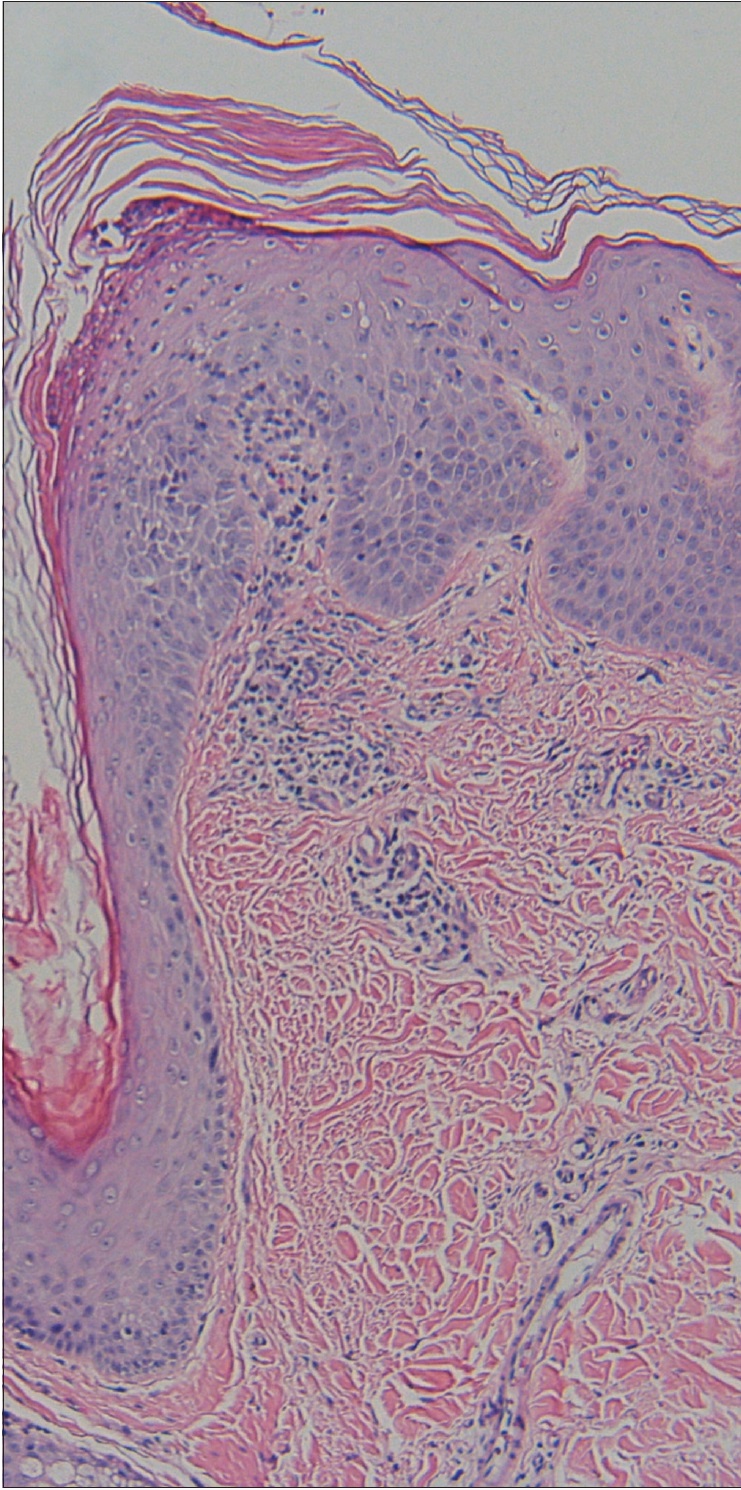 |
| Figure 3a: Biopsy of linear psoriasis on the upper back showing hyperkeratosis, acanthosis and elongation of rete ridges (H and E, ×100) |
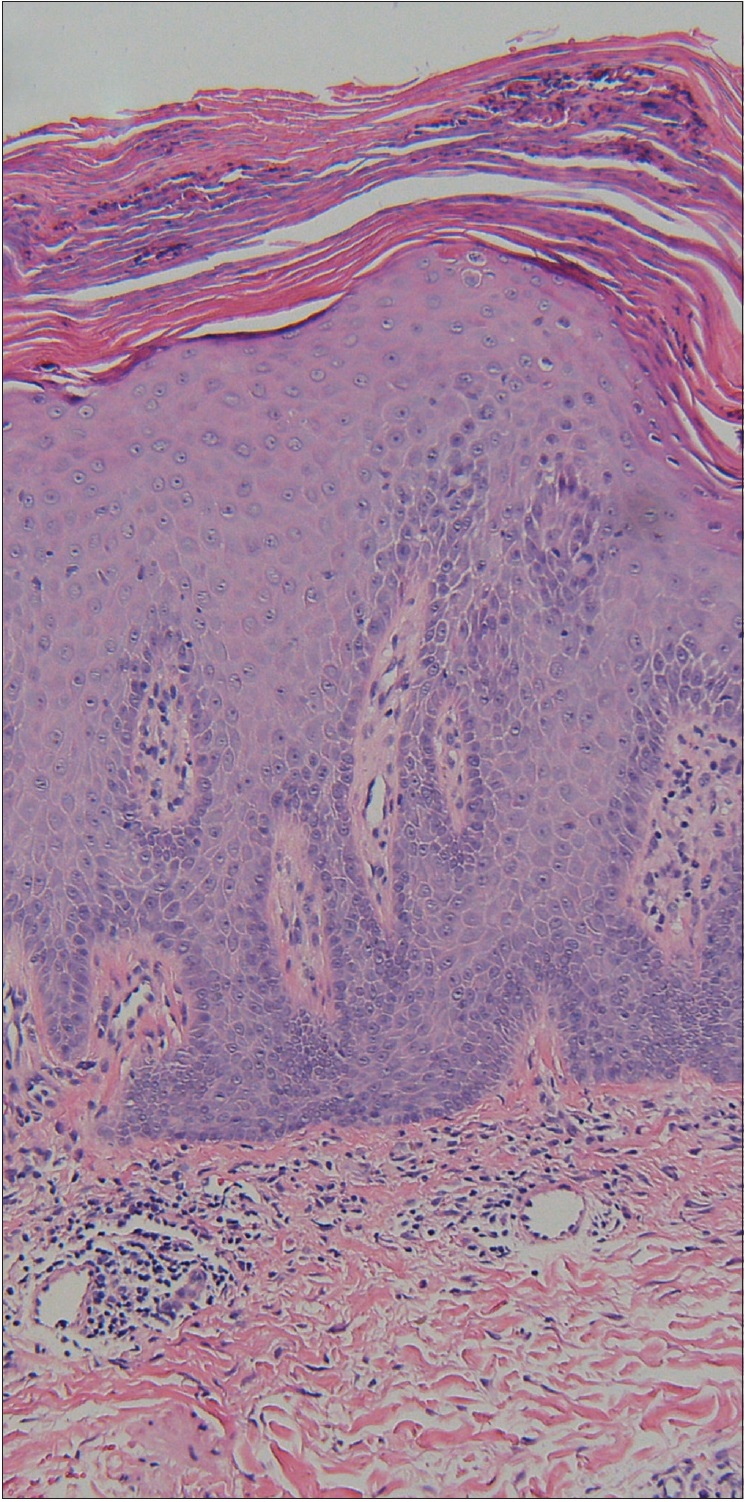 |
| Figure 3b: Biopsy of plaque psoriasis on the abdomen showing parakeratosis, acanthosis, elongation of rete ridges, Munro's micrabscesses and upper dermal infiltrate with lymphocytes and neutrophils (H and E, ×100) |
Our report is the first to demonstrate the effects of ustekinumab in the treatment of linear psoriasis. Ustekinumab is an anti-interleukin-23 agent with superior efficacy compared to etanercept in a controlled trial.[6] Although ustekinumab is approved for the treatment of plaque psoriasis and psoriatic arthritis, currently there has been no report of its use in the treatment of linear psoriasis. Previous reports of anti-tumor necrosis factor-α agents for the treatment of linear psoriasis all failed to show adequate response. These agents include infliximab, etanercept and adalimumab.[1],[7] The relatively inadequate treatment response of ustekinumab in linear psoriasis compared to plaque psoriasis underlines the importance of phenotyping for psoriasis to predict biologic responsiveness.[8] In addition, targeting other pathways may be of therapeutic potential for linear psoriasis.
The differential treatment responses are consistent with the hypothesis that linear psoriasis may be a special variant of psoriasis with a nevoid nature, which is distinct from plaque psoriasis. The exact nature of linear psoriasis is not known, but a postzygotic mutation has been proposed. Moreover, the age of onset of linear psoriasis is often delayed as in our case. However, in our patient, the onset of his linear psoriasis seemed to coevolve with his plaque psoriasis. The linear form became more prominent after the resolution of his plaque psoriasis. More studies are warranted to better understand the etiology as well as the treatment of linear psoriasis.
This work was supported by a grant from the National Taiwan University Hospital. The funders had no role in the study design, data collection and analysis, decision to publish or preparation of the manuscript.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
| 1. | Colombo L, Marconi M, Mapelli ET, Crespi E, Gualandri L, Menni S, et al. Superimposed linear psoriasis: Low effectiveness of biologic therapy. G Ital Dermatol Venereol 2011;146:311-3. [Google Scholar] |
| 2. | Kira M, Katayama I. Superimposed linear psoriasis. J Dermatol 2010;37:1063-5. [Google Scholar] |
| 3. | Kao PH, Hui RY, Yang CH, Huang YH. Effectiveness and safety of adalimumab in treating moderate to severe psoriasis patients with psoriatic arthritis in Taiwan. Dermatol Sin 2015;33:119-23. [Google Scholar] |
| 4. | Rott S, Küster RM, Mrowietz U. Successful treatment of severe psoriatic arthritis with infliximab in an 11-year-old child suffering from linear psoriasis along lines of Blaschko. Br J Dermatol 2007;157:191-2. [Google Scholar] |
| 5. | Larsen F, Menter A, Cockerell CJ, Wilcox BN. Verrucous linear (segmental) psoriasis of the right leg responding to radiation therapy. J Drugs Dermatol 2008;7:969-71. [Google Scholar] |
| 6. | Griffiths CE, Strober BE, van de Kerkhof P, Ho V, Fidelus-Gort R, Yeilding N, et al. Comparison of ustekinumab and etanercept for moderate-to-severe psoriasis. N Engl J Med 2010;362:118-28. [Google Scholar] |
| 7. | Arnold AW, Happle R, Itin PH. Superimposed linear psoriasis unmasked by therapy with adalimumab. Eur J Dermatol 2010;20:573-4. [Google Scholar] |
| 8. | Karczewski J, Poniedzialek B, Rzymski P, Adamski Z. Factors affecting response to biologic treatment in psoriasis. Dermatol Ther 2014;27:323-30. [Google Scholar] |
Fulltext Views
3,489
PDF downloads
1,725




