Translate this page into:
Retrospective analysis of basal cell carcinoma
Correspondence Address:
Sibel Hakverdi
Kuzeytepe Mah. Bah�elievler Sit, Kardelen Sk. No: 10, 31030- Antakya / Hatay
Turkey
| How to cite this article: Hakverdi S, Balci DD, Dogramaci CA, Toprak S, Yaldiz M. Retrospective analysis of basal cell carcinoma. Indian J Dermatol Venereol Leprol 2011;77:251 |
Abstract
Background: Basal cell carcinomas (BCCs) are the most prevalent cancer type among white-skinned populations worldwide. Aims: To analyze the gender and age-related incidence of basal cell carcinoma (BCC) histopathologic subtypes, to classify BCCs according to their anatomical location, invasion depth, and size, and to determine the relationship between BCC subtypes and margin of surgical excision. Methods: All BCCs analysed in our center between 2005 and 2010 were studied retrospectively. The samples, which were totally excised, were included on the basis of histopathological diagnosis of BCC, and confirmed by two pathologists. Patient data included sex, age at diagnosis, tumor location, histological subtypes, invasion depth, and size. Results: We recorded 197 BCCs obtained from 181 white patients (80 females, 101 males). The mean age among males was 64.11, and 59.33 among females. Of the cases, 45.17% were nodular, 22.33% were mixed, and 15.22 were infiltrative type. 91.84% of the cases were located on the head and neck, 3.04% were on the limbs, and 1.52 % were on the trunk. In 32 cases, the margin of surgical excision was positive (17.7%): nodular 12%, infiltrative 43.3%, mixed 20.6%, micronodular 10%, and superfacial multicentric 5.5%. Of these total 32 cases, 34.4% were located on the eyes region, 28.1% were found on the nose, and 15.6% were on the ears. Invasion depth of tumors varied from 0.5 to 22.125 mm. Conclusions: The results of our study exhibit differences in anatomical distribution, sex and mean age, invasion depth, and size of BCC subtypes. The recurrence rate for incompletely excised tumors varies according to the location and type of the tumor. Infiltrative tumors are more likely to recur and have positive margin of surgical excision. The highest positive margin of surgical excision is in infiltrative BCC. Tumors at difficult-to-treat sites and large and/or deeply invasive tumors are more liable to recur.Introduction
Basal cell carcinomas (BCCs) are the most prevalent cancer type among white-skinned populations worldwide, and particularly in industrialized Western societies. In addition, the incidence of skin cancers is rising all over the world. Geographical location plays an extremely important role in the distribution and frequency of incidence rates. Despite low mortality rates because of BCC, it is highly prevalent, and so it constitutes a significant and costly health problem. [1],[2]
BCC is a slow-developing malignant skin tumor, infiltrating the adjacent tissues, and ultraviolet (UV) radiation is accepted as one of the most important causal factors of BCCs. Exposure to ionizing radiation, exposure to chemical carcinogens, and possibly infection with human papilloma viruses, ethnical differences, type of skin, chronic irritation, chronic inflammation, burns, skin lesions, immunologic, and genetic factors are the other causal factors. [3],[4]
Head and neck are known as the most common localizations of BCC (80%), but the anatomical site distribution is different for the histologic subtypes of BCC: nodular BCC mostly occurs on the head and neck, whereas superficial BCC predominantly occurs on the trunk. Data received from these studies have also shown that the histological subtype most frequently occurring on the trunk is the superficial type and that all BCCs increasingly tend to occur on the trunk. [5]
BCCs generally occur in persons older than 50 years, but not much is known about its incidence in persons younger than 40 years. To date, studies which aimed to investigate BCC in the young have been unable to determine any trends. [6]
The specific aim of our study was to estimate the sex and age-related incidence of BCC in our center between 2005 and 2010, in a group of patients varying in age from 33 to 95 years. An additional aim was to classify BCC subtypes according to their location, invasion depth, and size. This study is important in that, to the best of our knowledge, it is the first study focusing primarily on the correlation between histologic subtypes of BCC and invasion depth and size of the tumors.
Methods
All BCCs analyzed in Mustafa Kemal University, School of Medicine, Hatay, Turkey, between 2005 and 2010 were studied retrospectively. The samples, which were totally excised, were included on the basis of histopathological diagnosis of BCC, and confirmed by two pathologists, following the permission of the head of our institution.
Patient and tumor characteristics were derived from patient records and pathology reports. Patient data included sex, age at diagnosis, tumor location, histological subtypes, invasion depth, and diameter (using Olympus Eyepiece Micrometer U-OCMC10/100XY). Multiple tumors were also included. Recurrent tumors were excluded.
Samples were re-evaluated to identify BCC histologic subtype. Besides biopsy reports, reports of surgical excisions, when available, were also included to evaluate the entire tumor. Histologically, BCCs were divided into nodular, superficial, infiltrative, morpheiform, metatypical, infundibulocystic, micronodular, keratotic (also known as "pilar BCC"), fibroepithelioma, and mixed types. When tumor cell clusters with various sizes and shapes, showing typical peripheral palisading, were embedded in the dermis, they were termed as nodular BCC [Figure - 1]. If these clusters displayed basaloid cells arranged as elongated strands, with a few thick layers and little or no palisading peripheral cells, they were termed as BCC of the infiltrative type [Figure - 2]. Superficial BCCs were those exhibiting buds and irregular proliferations of tumor cells attached to an unusually atrophic epidermis, and showing little or no penetration into the dermis [Figure - 3]. Morpheiform BCC had to show densely proplastic and heavily collagenized stroma, small irregular (shaply angulated) tongues of neoplastic basaloid cells, often 1-4 cells thick. Metatypical BCC (equated by some authors with "basosquamous carcinoma") is marked with infiltrating jagged tongues of tumor cells, some of which show an abortive peripheral palisade and neat basaloid morphology, admixed with other areas showing intercellular bridge formation and cytoplasmic keratinization. In the infundibulocystic BCC, proliferating basaloid cells, typically in continuity with overlying epidermis, are observed as rounded nests surrounding structures filled with keratin and lined by a stratified epithelium with a granular cell layer. Micronodular BCC manifests as uniformly small nests of neoplastic basal cells with rounded peripheral contours extending widely throughout the sampled dermis. The adjacent stroma shows fibroplasia [Figure - 4]. The keratotic BCC manifests as rounded large basaloid tumor nests which show central keratinization and degeneration. Fibroepithelioma manifests as atypical basaloid cells growing in thin lacy strands radiating down from points of continuity with the overlying epidermis. The stroma is often myxoid or shows plump stromal cells with collagens deposited around the basaloid tumor tongues. Some growth patterns which are explained above can occur in a combination, and this is called mixed type [4],[7],[8] [Figure - 5].
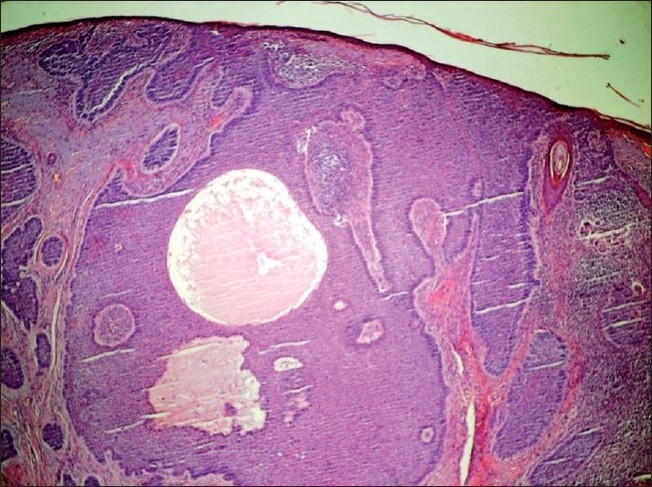 |
| Figure 1: Nodular BCC manifests multiple variable-sized and rounded nodules with a pushing contour in opposition to a stroma. The nodules of the tumor show a peripheral palisade of basaloid cells. (H and E, ×40) |
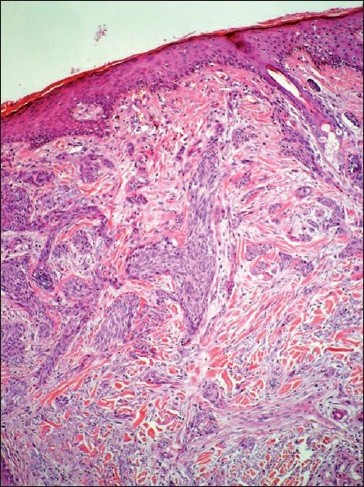 |
| Figure 2: BCC of the infiltrative type shows heavy stromal collagenization and proplasia stromal fibroblast. The tumor cell nests are variable in size and shape with jagged contours. (H and E, ×200) |
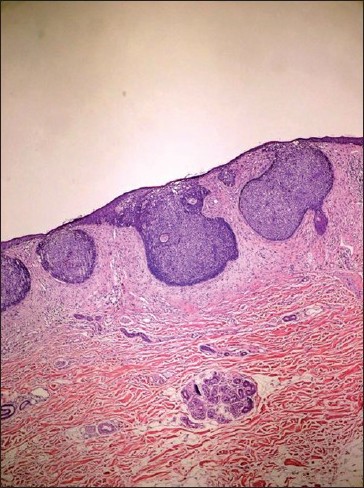 |
| Figure 3: Superficial BCC were those exhibiting buds and irregular proliferations of tumor cells attached to an atrophic epidermis, and showing little penetration into the dermis. (H and E, ×40) |
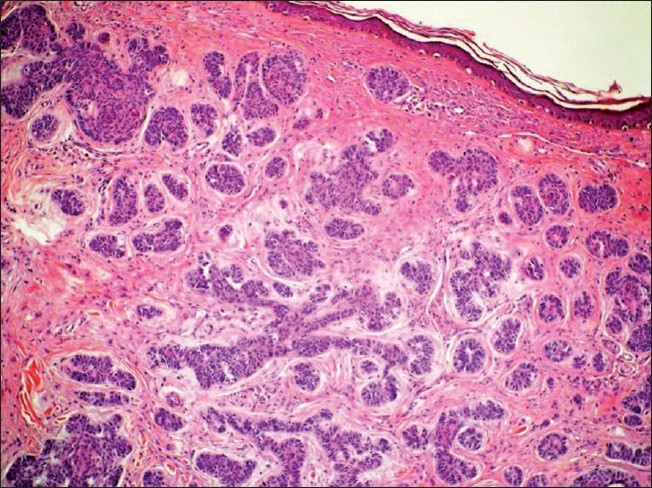 |
| Figure 4: Micronodular BCC manifests uniformly small nests of neoplastic basal cells with rounded peripheral contours extending widely throughout the dermis, and the adjecent stroma shows fibroplasia. (H and E, �40) |
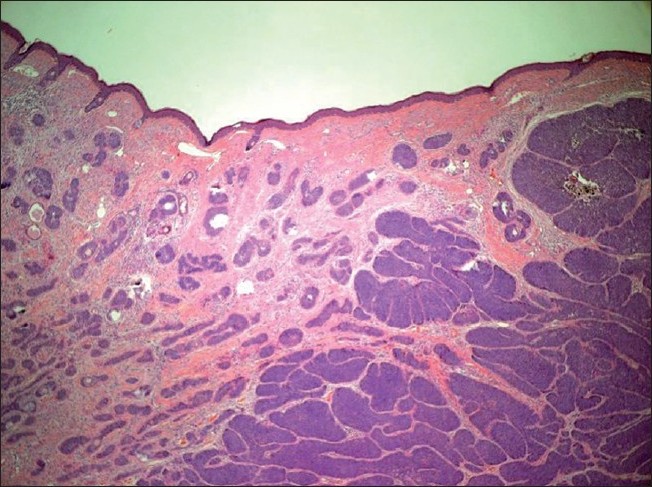 |
| Figure 5: Mixed-type BCC: a combination of nodular and micronodular BCC (H and E, ×40) |
Results
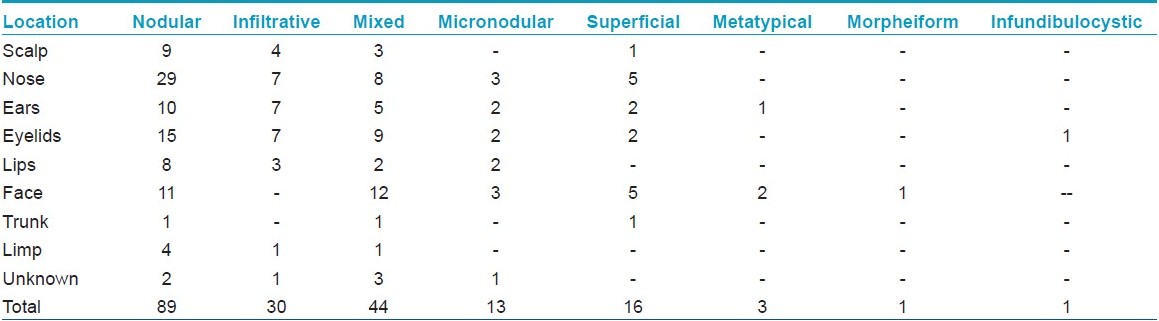
We recorded 197 BCCs obtained from 181 patients (all from white population) (80 females, 101 males). The mean age among male patients was 64.11, whereas in women it was 59.33, and in both sexes the highest frequency was 50-80 year age group. Among patients having multiple BCCs, 12 had two or more tumors. The highest number of BCC in a single patient was 5. There were 181 cases located on the head and neck (91.84 %), 3 cases were on the trunk (1.52%), and 6 cases were on the limbs (3.04%). The location was unknown in seven cases (3.55 %). The detailed anatomical distributions of BCCs according to their histologic subtypes are given in [Table - 1].
The global distribution of histopathological subtypes confirmed the predominance of the nodular type. There were 89 cases of nodular BCC (45.17 %), 44 cases of mixed type (22.33%), 30 cases of infiltrative type (15.22%), 16 cases of superficial BCC (8.12%), 3 cases of metatypical BCC (1.52%), 1 case of morpheiform BCC (0.5%), and 1 case of infundibulocystic BCC. The other subtypes of BCC were not observed. There was no histopathologically indeterminate BCC subtype.
In 32 cases, the margin of surgical excision was positive (17.7%): 10 of the 83 nodular BCC (12%), 13 of the 30 infiltrative BCC (43.3%), 7 of the 34 mixed BCC (20.6%), 1 of the 10 the micronodular BCC (10%), and 1 of the 18 the superficial multicentric BCC (5.5%). Of these total 32 cases, 11 were located on the eyes region (34.4%), 9 were found on the nose (28.1%), 5 were on the ears (15.6%), 3 were on the lips (9.4%), 3 were on the scalp (9.4%), and 1 was in the gluteal region (3.1%).
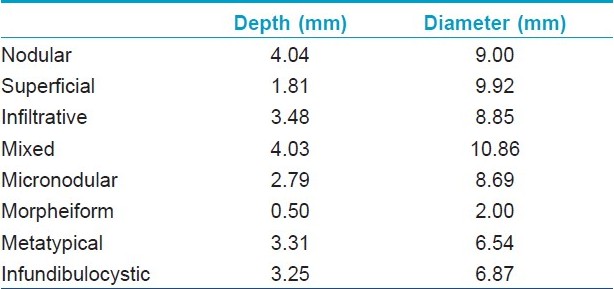
The smallest tumor was 1 mm in diameter, and the largest was 4.3 cm. The invasion depth of tumors varied from 0.5 to 22.125 mm. The nodular BCC had the highest mean invasion depth (4.04 mm), followed by mixed-type BCC (4.03 mm), and infiltrative BCC (3.48 mm) and the smallest was morpheic BCC (0.5 mm). The mean size of the tumors according to BCC subtypes was largest in mixed-type BCC (10.86 mm) and the smallest in morpheic BCC (2.0 mm). Although the deepest tumor was found in nodular BCC and the largest size was in mixed-type BCC, positive surgical margin was in infiltrative type BCC. The mean depth and size of the tumors according to each BCC histologic subtype are presented in [Table - 2].
Discussion
BCC is the most common form of cancer worldwide, and the incidence of this cancer is increasing. As the cost of its treatment constitutes a big burden on economies of countries, this cancer type should be analyzed in detail in terms of causes, age and gender distribution, localization, margin of excision, recurrence rates, and subtypes. [1],[2]
Age and sex distribution
In previous studies, it has been found that the frequency of BCC in females is lower than in men. As regards the distribution of BCC, Yaldiz. [9] et al, found that of the patients, 62.8% were males, Bastiaens et al,[10] found it as 54%, and Raasch [5] as 58.6%. Our findings confirm these data with 55.8% of our patients being male.
The results of our study exhibit different patterns of age-related incidence rates for BCC subtypes in males and females. The age-related incidence rate in females begins in the early 30s, though rare, and rises to a peak in the 40- to 49-year age group, and then generally remains steady, compared with a slow but steady rise until 70- to 79-year age group in males. [5] In our study, the mean age among male patients was 64.11, whereas in women the mean age was lower (59.33), with the highest frequency being between 50 and 80 year age group in both sexes. This study supports previous findings that in females BCC begins at a younger age than in men.
Anatomical distribution
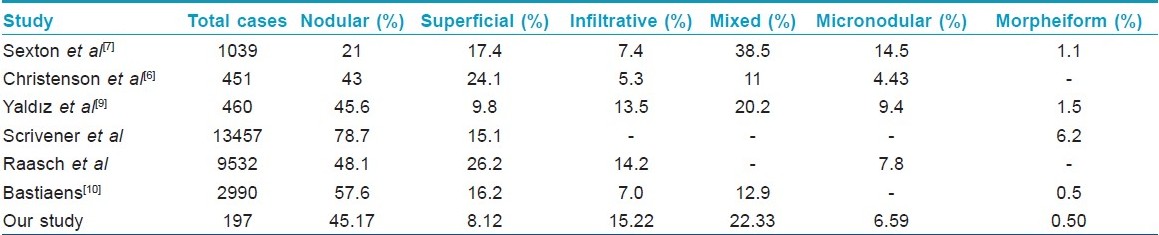
The distribution of the histologic subtypes in our population confirms that nodular BCC is the most frequent subtype (45.17%), followed by mixed type (22.33%) and infiltrative type (15.22%). In contrast to the findings in other studies as regards the high frequency of superficial BCC, we found that it is not so common among our population (8.12%). The age-specific incidence rates for nodular BCC, showing a dramatic and progressive increase with age in both males and females, support previous speculation that the nodular subtype is more related to chronic cumulative sun exposure. [5],[11] One reason for the lower frequency of superficial BCCs might be that they are predominantly observed on sun-protected areas of the body, as noted by Scrivener et al, and Puavilai et al,. [12],[13] The frequency of BCC subtypes in the literature is presented in [Table - 3].
The main location of our BCC with almost all subtypes was almost the head and neck region: 181 of the total cases we examined (91.84%) were in the head and neck region, 9 cases (4.56%) were on the trunk and limbs, and 7 cases (3.55%) could not be located. In contrast to the findings presented in other studies, which state that superficial BCC predominantly occur on the trunk. [5],[12] The cases in our study were mainly located in the head and neck region.
Size, depth and margins
Metastases are rare and mostly are said to correlate more closely to the size and depth, and less to the histologic subtype of the original tumor. [4],[14],[15],[16] However, in our study, we found that there is a more significant correlation histologic subtype of the original tumor rather than its size and depth. Metastases are expected to occur when large tumors greater than 3 cm in diameter are present. Whereas the risk of metastases is 1- 2% in tumors of 3 cm diameter, this risk increases to 20 -25% in 5 cm, and up to 50% in lesions greater than 10 cm in diameter. [17] If a BCC is greater than 10 cm in diameter, it is called "giant" and poses a significant risk of morbidity and mortality. [4],[15],[16]
In our study, the margin of surgical excision was positive in 17.7% of the cases, infiltrative BCC being the most common subtype BCC (43.3%), followed by mixed-type BCC (20.6%) and nodular BCC (12%). The most common anatomical site for the margin of surgical excision positivity was the eye region (34.37%) followed by the nose (25%), and the ears (15.6%). The recurrence rate for incompletely excised tumors varies according to the location and type of the tumor. Infiltrative tumors, which are accepted to have aggressive nature, are more likely to recur and have positive margin of surgical excision. [18],[19],[20],[21] We also found that the highest positive margin of surgical excision was in infiltrative BCC. Classification according to anatomical site is also important in the determination of positivity of surgical excision margin. Tumors at some sites, e.g. nose, ears, eyes, are difficult to treat and therefore more liable to recur. [18],[22] In addition, if tumors are large and/or deeply invasive, they may be resistant to treatment and more likely to recur at a later period. [17],[18] Our findings as regards the relationship between location and positivity in the margin of surgical excision comply with these facts.
To sum up, in this study, we have found some important results: (1) BCC was more frequent in males ( and shows a trend to occur in younger ages); (2) unlike the findings in other studies, the location of superficial BCC was not the trunk, but the head and neck region; (3) as regards the most frequently observed BCC subtypes, superficial BCC was not as high as reported in other studies; and (4) although the deepest tumor was found in nodular BCC and the largest size was in mixed-type BCC, the highest positive margin of surgical excision was in infiltrative BCC.
In conclusion, the histologic tumor subtype is often a factor used by the clinician in their decision regarding the management of BCC. Therefore, it is the duty of pathologists to give a detailed report of these subtypes. The approach to therapy for skin cancer plays an important role in the potential recurrence of that tumor. If the tumor subtypes are aggressive, they usually require more decisive treatment. Therefore, the frequency of BCC subtypes, their depth and size, and anatomical locations, which change according to various factors, should be analyzed, as we have done in this study, for many different regions in the world so as to gain a deeper and more wholesome understanding of the distribution of skin cancer so that more effective ways of combating it can be implemented.
| 1. |
Brewster DH, Bhatti LA, Inglish JHC, Nain ER, Doherty VR. Recent trends in incidance of nonmelanoma skin cancer in the East of Scotland, 1992-2003. Br J Dermatol 2007;156:1295-300.
[Google Scholar]
|
| 2. |
Hoey SE, Devereux CE, Murray L, Catney D, Gavin A, Kumar S, et al. Skin cancer trends in Northern Ireland and consequences for provision of dermatology services. Br J Dermatol 2007;156:1301-7.
[Google Scholar]
|
| 3. |
Pfister H, Ter Schegget J. Role of HPV in cutaneous premalignant and malignant tumors. Clin Dermatol 1997;15:335-47.
[Google Scholar]
|
| 4. |
Crowson AN. Basal cell carcinoma: Biology, morphology and clinical implications. Modern Pathology 2006;19:127-47.
[Google Scholar]
|
| 5. |
Raasch BA, Buettner PG, Garbe C. Basal cell carcinoma: Histological classification and body-site distribution. Br J Dermatol 2006;155:401-7.
[Google Scholar]
|
| 6. |
Christenson LJ, Borrowman TA, Vachon CM, Tollefson MM, Otley CC, Weaver AL, et al. Incidance of basal cell and squamous cell carcinomas in a population younger than 40 years. JAMA 2005;294:681-90.
[Google Scholar]
|
| 7. |
Sexton M, Jones DB, Maloney ME. Histologic pattern analysis of basal cell carcinoma. Study of a series of 1039 consecutive neoplasms. Am J Acad Dermatol 1990;23:1118-26.
[Google Scholar]
|
| 8. |
Cohen PR, Schulze KE, Nelson BR. Basal cell carcinoma with mixt histology: A possible pathogenesis for reccurent skin cancer. Dermatologic Surg 2006;32:542-51.
[Google Scholar]
|
| 9. |
Yaldýz M, Uzunlar AK, Yýlmaz F, Buyukbayram H, Kýlýnç N, Arslan A. Histopathologic features of the 460 basal cell carcinoma cases. J of Med Sci 1999;19:249-54.
[Google Scholar]
|
| 10. |
Bastiaens MT, Hoefnagel JJ, Bruijn JA, Westendorp RG, Vermeer BJ, Bavinck BN. Differences in age, site distribution, and sex between nodular and superficial basal cell carcinomas indicate different types of tumors. J Invest Dermatol 1998;110:880-4.
[Google Scholar]
|
| 11. |
Cohen PR, Schulze KE, Nelson BR. Cutaneous carcinoma with mixt histology: A potential etiology for skin cancer recurrence and an indication for Mohs microscopically controlled surgical excision. South Med J 2005;98:240-7.
[Google Scholar]
|
| 12. |
Scrivener Y, Grosshans E, Cribier B. Variations of basal cell carcinomas according to gender, age, location and histopathologic subtype. Br J Dermatol 2002;147:41-7.
[Google Scholar]
|
| 13. |
Puavilai S, Sirapan S. Correlation of histological subtypes of basal cell carcinoma with age, sex and distribution of skin lesion: A five-year study at Ramathibody Hospital. J Med Assoc Thai 2002;85:560-4.
[Google Scholar]
|
| 14. |
Lo JS, Snow SN, Reizner GT. Metastatic basal cell carcinoma: Report of twelve cases with a review of the literature. J Am Acad Dermatol 1991;24:715-9.
[Google Scholar]
|
| 15. |
Sahl WJ. Basal cell carcinoma: Influence of tumor size on mortality and morbidity. Int J Dermatol 1995;34:319-21.
[Google Scholar]
|
| 16. |
Randle HW. Basal cell carcinoma: Identification and treatment of the high-risk patient. Dermatol Surg 1996;22:255-61.
[Google Scholar]
|
| 17. |
Snow SN, Sahl WJ, Lo J. Metastatic basal cell carcinoma: Report of 5 cases. Cancer 1994;73:328-35.
[Google Scholar]
|
| 18. |
Rippey JJ. Why classify basal cell carcinomas? Histopathology 1998;32:393-8.
[Google Scholar]
|
| 19. |
Emmett AJ. Sugical analysis and biological behavior of 2277 basal cell carcinomas. Aust N Z J Surg 1990;60:855-63.
[Google Scholar]
|
| 20. |
Sloane JP. The value of typing basal cell carcinomas in predicting recurrence after surgical excision. Br J Dermatol 1977;96:127-32.
[Google Scholar]
|
| 21. |
Orengo IF, Salasche SJ, Fewkes J, Khan J et al. Correlation of histologic subtypes of basal cell carcinoma and number of Mohs stages required to achieve a tumor-free plane. J Am Acad Dermatol 1997;37:395-7.
[Google Scholar]
|
| 22. |
Dixon AY, Lee SH, McGregor DH. Factors predictive of recurrence basal cell carcinoma. Am J Dermatopathol 1989;11:222-32.
[Google Scholar]
|
Fulltext Views
4,919
PDF downloads
4,227





![[Figure - 1]](#fig_ijdvl_2011_77_2_251_77483_f4.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2011_77_2_251_77483_f5.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2011_77_2_251_77483_f6.jpg){kind=link}
![[Figure - 4]](#fig_ijdvl_2011_77_2_251_77483_f7.jpg){kind=link}
![[Figure - 5]](#fig_ijdvl_2011_77_2_251_77483_f8.jpg){kind=link}
![[Table - 1]](#tbl_ijdvl_2011_77_2_251_77483_t1.jpg){kind=link}
![[Table - 2]](#tbl_ijdvl_2011_77_2_251_77483_t2.jpg){kind=link}
![[Table - 3]](#tbl_ijdvl_2011_77_2_251_77483_t3.jpg){kind=link}