Translate this page into:
Reversible hyperpigmentation as the first manifestation of dietary vitamin B12 deficiency
2 Department of Dermatology, All India Institute of Medical Sciences, New Delhi, India
Correspondence Address:
Sanjay Singh
C-9, New Medical Enclave, Banaras Hindu University, Varanasi - 221 005
India
| How to cite this article: Srivastava N, Chand S, Bansal M, Srivastava K, Singh S. Reversible hyperpigmentation as the first manifestation of dietary vitamin B12 deficiency. Indian J Dermatol Venereol Leprol 2006;72:389-390 |
 |
| Pretreatment (a) and post-treatment (b) (8 weeks) photographs of palms and soles |
|
| Pretreatment (a) and post-treatment (b) (8 weeks) photographs of palms and soles |
Sir,
Vitamin B 12 deficiency is considered to be rare and presents with different combinations of neurological manifestations, hematological changes, discoloration of skin, hair and nails, weakness, syncope and diarrhea. Common cause of vitamin B 12 deficiency is malabsorption, usually due to pernicious anemia or gastric resection and rarely inadequate intake.[1] Inadequate intake almost exclusively occurs in strict vegetarians. Hyperpigmentation of skin has been reported only rarely as the presenting manifestation of vitamin B 12 deficiency.[2] There is only one such Indian report.[3]
A 34-year-old Indian male presented with darkening of skin and discoloration of hair and nails for two months. Darkening initially started on the palms and feet [Figure - 1] and then gradually involved the face, gums and tongue. He also complained of diarrhea, decreased appetite, weakness and significant weight loss for one and a half months. There was history of similar episode of diarrhea and pigmentation two years back, which responded to multivitamins in a few months. There was no history of chronic illness. Patient′s diet was strictly vegetarian and he used to take milk occasionally. On systemic examination the only significant finding was pallor.
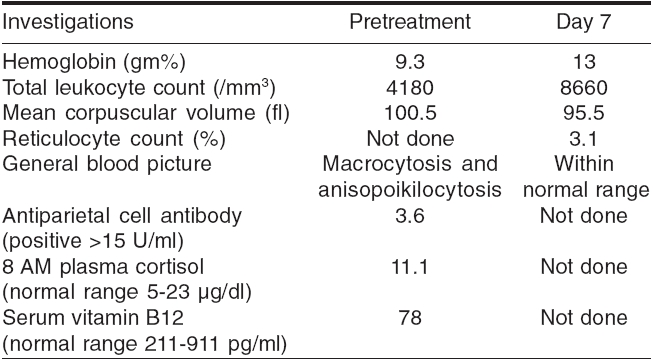
Hematological and special investigations were performed [Table - 1]. Skin biopsy showed increased melanin in the epidermis. Upper gastrointestinal endoscopy was normal and histopathological examination of the second part of the duodenum showed normal mucosa. Antiparietal cell antibody was negative. Diagnosis of hyperpigmentation due to vitamin B 12 deficiency was established. Patient was prescribed intramuscular injection of vitamin B 12 (1000 mg) daily for ten days, then weekly for one month and then monthly for two months. Subsequently, the patient has been receiving a multivitamin tablet daily containing vitamin B 12 (15 mg) for the past three months.
The patient′s hematological profile approached normal limits within one week of treatment [Table - 1]. Patient noticed improvement in subjective symptoms (diarrhea, malaise and fatigue) within two weeks and reversal in pigmentation initially on face and then on palms and feet within eight weeks. There has been no recurrence. The characteristic dermatological sign of vitamin B 12 deficiency is cutaneous pigmentation, which can be reversed by administration of vitamin B 12 .[4] Increased cutaneous pigmentation is especially accentuated in palmar creases, on the dorsa of hands and feet, in intertriginous areas, on oral mucosa and in recent scars. The mechanism of hyperpigmentation is unexplained. The most frequent cause of the deficiency is pernicious anemia.[1] The only Indian report of cutaneous hyperpigmentation due to vitamin B 12 deficiency is of a ten-month-old male child who was exclusively breastfed till three months of age and thereafter received diluted cow′s milk and occasional cereals.[3] Although the authors do not mention the cause of deficiency, it appears to be inadequate dietary intake. A few reports have suggested that vitamin B 12 deficiency may in fact be commoner than is generally thought.[5] Under-diagnosis of this condition may reflect a firmly held notion among doctors that the disease is rare.[5] Our report suggests that it may be worthwhile to consider the possibility in a patient with unexplained pigmentary changes. Early detection and adequate treatment will also prevent partially irreversible neurological manifestations.
| 1. |
Bernard M, Babior H, Franklin B. Megaloblastic anemias. In : Harrison's Principles of Internal Medicine. Kasper DL, Braunwald E, Fauci AS, Hauser SL, Longo DL, Jameson JL, editors. 16th ed. McGraw-Hill: New York; 2005. p. 601-7.
[Google Scholar]
|
| 2. |
Hoffman CF, Palmer DM, Papadopoulos D. Vitamin B12 deficiency: A case report of ongoing cutaneous hyperpigmentation. Cutis 2003;71:127-30.
[Google Scholar]
|
| 3. |
Ahuja SR, Sharma RA. Reversible cutaneous hyperpigmentation in vitamin B12 deficiency. Indian Pediatr 2003;40:170-1.
[Google Scholar]
|
| 4. |
Lee SH, Lee WS, Whang KC, Lee SJ, Chung JB. Hyperpigmentation in megaloblastic anemia. Int J Dermatol 1988;27:571-5.
[Google Scholar]
|
| 5. |
Wadia RS, Bandishti S, Kharche M. B12 and folate deficiency: incidence and clinical features. Neurol India 2000;48:302-4.
[Google Scholar]
|
Fulltext Views
16,513
PDF downloads
1,839





![[Figure - 1]](#fig_ijdvl_2006_72_5_389_27766_1.jpg){kind=link}
![[Table - 1]](#tbl_ijdvl_2006_72_5_389_27766_2.jpg){kind=link}