Translate this page into:
Scleredema adultorum of Buschke: With unusual manifestations in a young female
2 Department of Rheumatology, SRM Medical College and Research Centre, SRM University, Kattangaluthur-603203, India
Correspondence Address:
Kavitha Mohanasundaram
B 404, Staff quarters, SRM Medical College and Research Centre, SRM University, Kattangaluthur-603203
India
| How to cite this article: Mohanasundaram K, Kumarasamy S, Kumar R, Rajendran CP. Scleredema adultorum of Buschke: With unusual manifestations in a young female. Indian J Dermatol Venereol Leprol 2012;78:503-505 |
Sir,
Scleredema is a scleroderma like fibrosing disorder of the skin with no major morbidities, and systemic manifestations are rare in type 1 scleredema (adultorum of Buschke). We report a case of scleredema, presenting with dysphagia and hoarseness of voice resulting from esophageal dysmotility and vocal cord edema, respectively, both of which are uncommon manifestations. Though the benign nature of the disease is the rule in most cases, the systemic involvement has to be looked for and appropriately treated to prevent morbidity and mortality in scleredema adultorum of Buschke.
A 17-year-old girl was admitted with the history of progressive skin thickening, [Figure - 1] involving the face, neck, thorax and abdomen over a period of 1 month. Patient had sore throat and fever, 10 days prior to the onset of skin thickening, which subsided with antibiotics. She then developed hoarseness of voice and progressive dysphagia. There was no history of cough, dyspnea, nasal regurgitation or gastroesophageal reflux. Clinical examination showed thickened skin with induration in the face, neck, chest, back, arms and forearms. Skin was normal in fingers and toes. Cardiovascular, respiratory and central nervous system were clinically normal. No clinical evidence of proximal muscle weakness. With this clinical presentation, a provisional diagnosis of scleredema was made. Her complete blood count was normal with hemoglobin of 12.6 gm/dL total count of 5800 cells/cu.mm, differential count of polymorphs 63%, lymphocytes 35%, eosinophils 2%, platelet count of 2,85,000/cu.mm and ESR of 48 mm/hr. Throat swab culture yielded no growth. Anti-streptolysin O titre was negative, CRP was negative and creatine kinase was 45 IU/L. Blood sugar fasting and postprandial was found to be 85 mg/dL and 116 mg/dL, respectively. Liver and renal function test were within normal limits. Serum protein electrophoresis was normal. Electrocardiogram, echocardiogram, chest X-Ray and HRCT of chest were normal. Anti nuclear antibodies, anti-topoisomerase-1, anticentromere antibodies and anti U 1 RNP were negative. Skin biopsy showed mucinous deposit in dermis on alcian blue staining [Figure - 2], thickening of dermis with preserved appendages [Figure - 3], suggestive of scleredema. Videolaryngoscopy was done, which revealed bilateral vocal cord edema with interarytenoid thickening [Figure - 4]. Upper gastrointestinal endoscopy showed reduced motility in the upper portion of esophagus. The patient was treated with penicillin and methylprednisolone orally. The hoarseness of voice and difficulty in swallowing improved.
 |
| Figure 1: Skin thickening in scleredema |
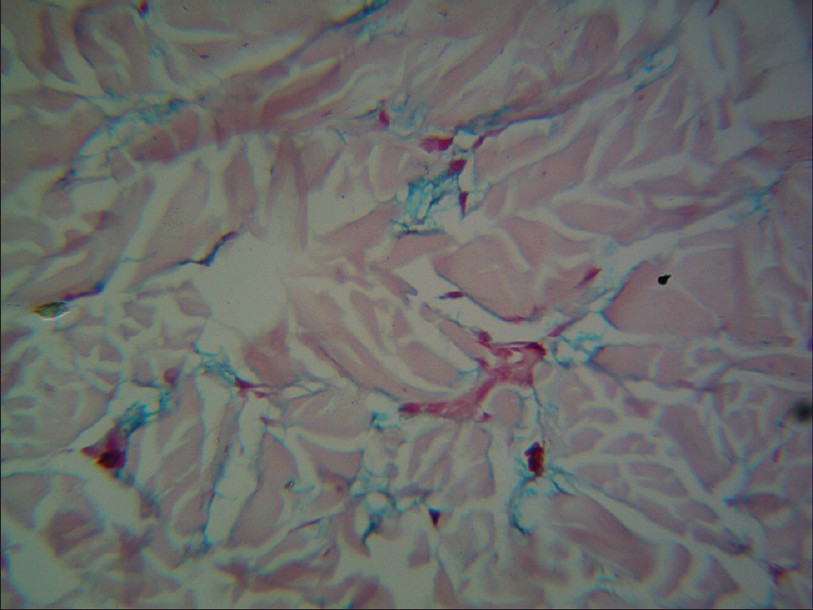 |
| Figure 2: Mucinous deposits in alcian blue staining of skin biopsy (H and E, ×400) |
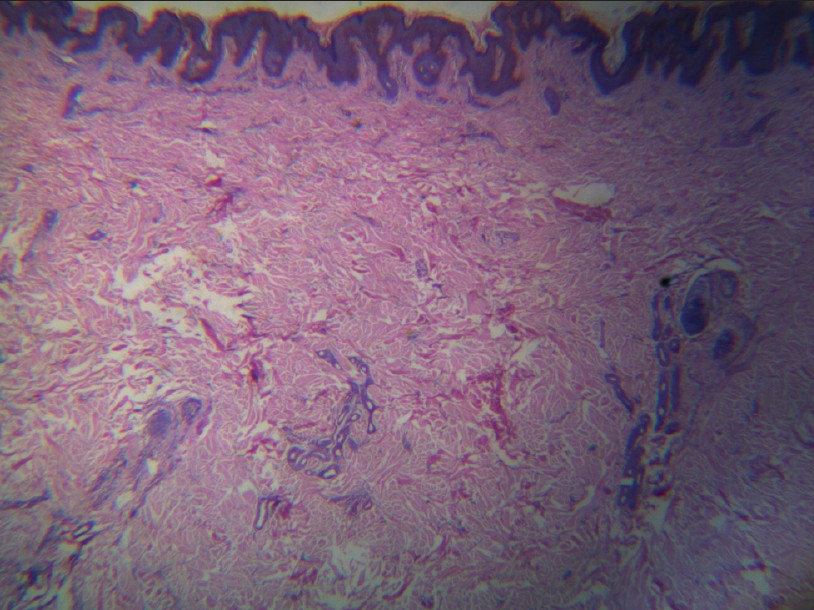 |
| Figure 3: Preserved appendages in skin biopsy (H and E, ×40) |
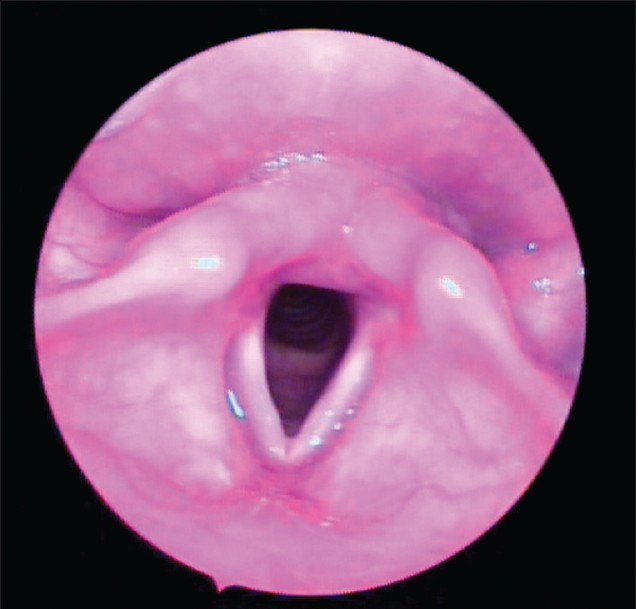 |
| Figure 4: Interarytenoid thickening in vocal cord |
Scleredema is a fibrosing disorder in which progressive thickening and hardening of the skin occurs. This usually starts behind the ears and slowly involves neck, face, shoulders, chest, upper back and finally whole body including limbs, sparing the digits. Scleredema is classified into 3 clinical types. Type 1 occurs following a streptococcal pharyngitis, [1] type 2 in patients with paraproteinemia [2] and type 3 in patients with diabetes (Krakowski type, scleredema diabeticorum). Type 1 scleredema is referred to as adultorum of Buschke since the post-infectious form of scleredema was the one, first described by Buschke himself. Systemic manifestations occur commonly in type 2 and type 3 but rare in type 1 scleredema.
Histopathological examination of skin biopsy in scleredema shows thickening of dermis with deposition of mucin and collagen with maintained ductal structures. [3] Even though it is a benign disease, it may cause death when internal organs are involved. The extra dermatological manifestations that have been reported are the involvement of tongue, upper part of esophagus, ocular muscles, pharynx, parotid gland, pleurae, peritoneum, spleen and the heart. [4] Involvement of upper esophagus resulting in aspiration has been reported. [5] Myocarditis and cardiac dysfunction have occurred in one patient. Our patient had involvement of vocal cord as evidenced by videolaryngoscopy with inter arytenoids thickening. Decreased motility in upper part of esophagus was observed in upper gastro-intestinal endoscopy. The involvement of vocal cord has lead to hoarseness of voice, and it was successfully treated with methyl prednisolone. Even after extensive searches of literature, we have found that vocal cord involvement in scleredema is unreported till date. As of our knowledge, this is the first case of scleredema adultorum of Buschke with involvement of vocal cords.
The treatment protocol for scleredema adultorum has not been effectively described in the literature. Steroids and immunomodulators have been tried for systemic involvement of this disease. Scleredema, often thought to be a benign disease, can rarely present with medical emergencies as was the case with our patient. Patients with scleredema have to be screened for internal organ involvement to prevent mortality.
| 1. |
Beers WH, Ince A, Moore TL. Scleredema adultorum of Buschke: A case report and review of the literature. Semin Arthritis Rheum 2006;35:355-9.
[Google Scholar]
|
| 2. |
Salisbury JA, Shallcross H, Leigh IM. Scleredema of Buschke associated with multiple myeloma. Clin Exp Dermatol 1988;13:269-70.
[Google Scholar]
|
| 3. |
Tasanen K, Palatsi R, Oikarinen A. Demonstration of increased levels of type I collagen mRNA using quantitative polymerase chain reaction in fibrotic and granulomatous skin diseases. Br J Dermatol 1998;139:23-6.
[Google Scholar]
|
| 4. |
Ulmer A, Schaumburg-Lever G, Bauer J, Kötter I, Fierlbeck G. Scleredema adultorum Buschke. Case report and review of the literature. Hautarzt 1998;49:48-54.
[Google Scholar]
|
| 5. |
Wright RA, Bernie H. Scleredema adultorum of Buschke with upper esophageal involvement. Am J Gastroenterol 1982;77:9-11.
[Google Scholar]
|
Fulltext Views
5,120
PDF downloads
1,712





![[Figure - 1]](#fig_ijdvl_2012_78_4_503_98090_u1.jpg){kind=link}
![[Figure - 2]](#fig_ijdvl_2012_78_4_503_98090_u2.jpg){kind=link}
![[Figure - 3]](#fig_ijdvl_2012_78_4_503_98090_u3.jpg){kind=link}
![[Figure - 4]](#fig_ijdvl_2012_78_4_503_98090_u4.jpg){kind=link}